Kanters Steve, Renaud Francoise, Rangaraj Ajay, Zhang Kenneth, Limbrick-Oldfield Eve, Hughes Monica, Ford Nathan, Vitoria Marco
School of Population and Public Health, University of British Columbia, 2206 E Mall, Vancouver, British Columbia, Canada.
RainCity Analytics, Vancouver, Canada.
EClinicalMedicine. 2022 May 12;48:101412. doi: 10.1016/j.eclinm.2022.101412. eCollection 2022 Jun.
This systematic review aimed to compare body weight gain associated outcomes over time between dolutegravir (DTG)-based antiretroviral (ART) regimens to other ART regimens, to compare tenofovir alafenamide (TAF)-based regimens, and to evaluate the associated prognostic factors.
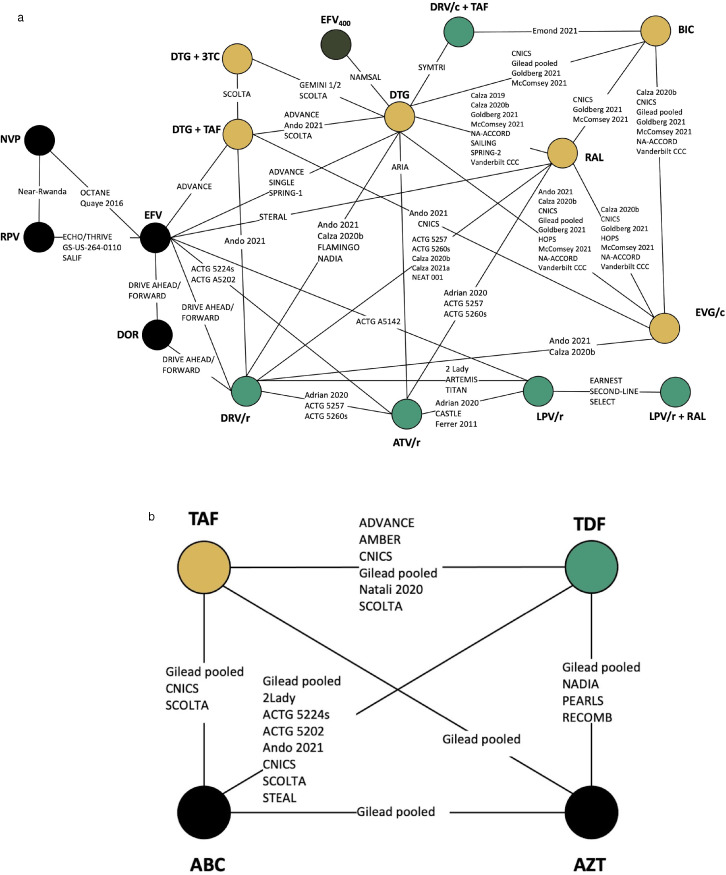
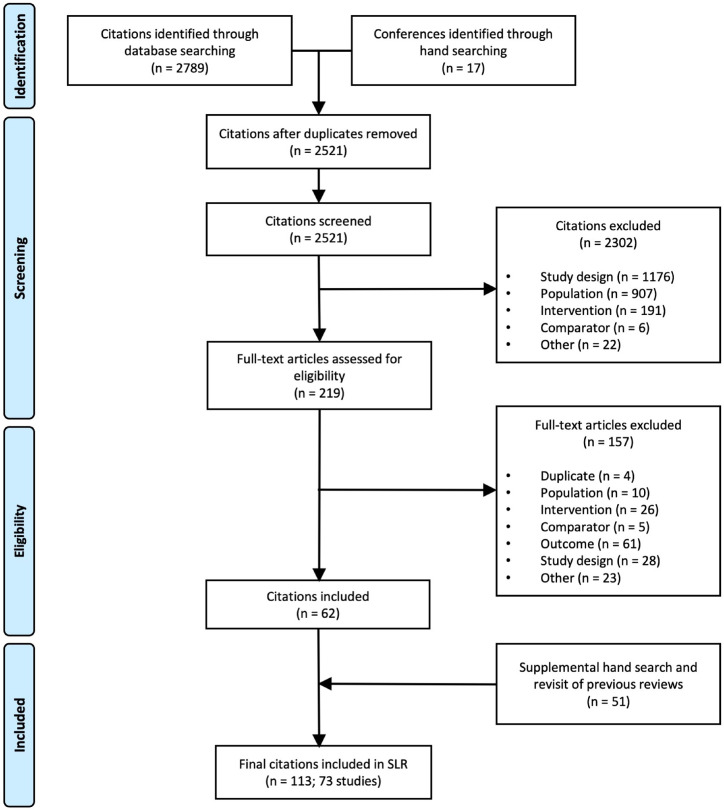
Systematic searches of MEDLINE, Embase, and CENTRAL for RCTs and observational studies comparing ART regimens were conducted on 13 September 2021. Outcomes of interest included: change in body weight, body mass index (BMI), waist circumference; and risk of hyperglycaemia and diabetes. Network meta-analyses were conducted at 12, 24, 48, 96 and 144 weeks using two networks differentiated by 3rd agents and backbone agents.
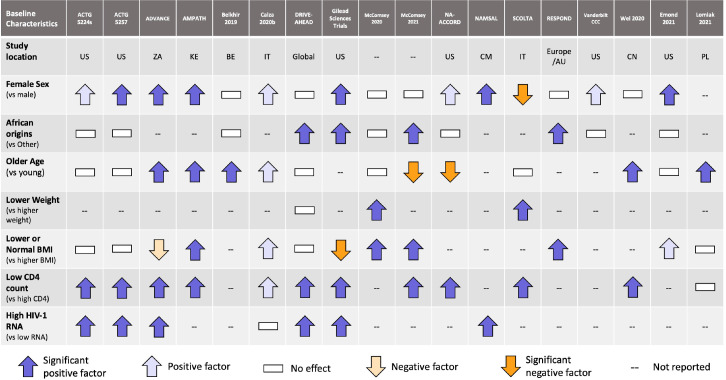
The review identified 113 publications reporting on 73 studies. DTG-based regimens led to statistically higher weight gains than efavirenz-based regimens at all time points (mean difference: 1·99 kg at 96 weeks; 95% credible interval: 0·85-3·09) and was higher over time than low-dose efavirenz-, elvitegravir-, and rilpivirine-based regimens. They were comparable to raltegravir-, bictegravir- and atazanavir-based regimens. For backbones, TAF led to higher weight gain relative to tenofovir disoproxil fumarate (TDF), abacavir, and zidovudine. Prognostic factor analysis showed both low CD4 cell count and high HIV RNA viral load at baseline were consistently associated with higher weight gain, while sex was an effect modifier to African origins.
DTG-based regimens lead to larger average weight gains than some other ART regimens and TAF leads to larger average weight gains than all other backbone antiretrovirals. Further research is needed to better understand long-term outcomes and their relationship to other metabolic outcomes.
The WHO Global HIV, Hepatitis and Sexually Transmitted Infections Programmes.
本系统评价旨在比较基于多替拉韦(DTG)的抗逆转录病毒(ART)方案与其他ART方案随时间推移的体重增加相关结局,比较基于替诺福韦艾拉酚胺(TAF)的方案,并评估相关的预后因素。
2021年9月13日,对MEDLINE、Embase和CENTRAL进行系统检索,以查找比较ART方案的随机对照试验(RCT)和观察性研究。感兴趣的结局包括:体重变化、体重指数(BMI)、腰围;以及高血糖和糖尿病风险。使用由第三代药物和主干药物区分的两个网络,在第12、24、48、96和144周进行网络荟萃分析。
该评价共纳入113篇报道73项研究的文献。在所有时间点,基于DTG的方案导致的体重增加在统计学上均高于基于依非韦伦的方案(96周时平均差异:1.99kg;95%可信区间:0.85 - 3.09),且随时间推移高于基于低剂量依非韦伦、埃替格韦和利匹韦林的方案。它们与基于拉替拉韦、比克替拉韦和阿扎那韦的方案相当。对于主干药物,相对于富马酸替诺福韦二吡呋酯(TDF)、阿巴卡韦和齐多夫定,TAF导致体重增加更多。预后因素分析表明,基线时低CD4细胞计数和高HIV RNA病毒载量均与更高的体重增加持续相关,而性别是非洲裔人群体重增加的效应修饰因素。
基于DTG的方案比其他一些ART方案导致更大的平均体重增加,TAF比所有其他主干抗逆转录病毒药物导致更大的平均体重增加。需要进一步研究以更好地了解长期结局及其与其他代谢结局的关系。
世界卫生组织全球艾滋病毒、肝炎和性传播感染规划。