Zheng Zhou, Yu Qingsheng, Peng Hui, Zhang Wanzong, Shen Yi, Feng Hui, Huang Long, Zhou Fuhai, Zhang Qi, Wang Qin
The First Affiliated Hospital of Anhui University of Chinese Medicine, Hefei, China.
Institute of Chinese Medicine Surgery, Anhui Academy of Chinese Medicine, Hefei, China.
Front Surg. 2022 May 30;9:834466. doi: 10.3389/fsurg.2022.834466. eCollection 2022.
Splenectomy is one crucial solution for hypersplenism with portal hypertension. However, portal vein system thrombosis (PVST) caused by hemodynamic changes affects the prognosis of patients. We analyze the changes in portal vein hemodynamics following splenectomy for Wilson's disease combined with portal hypertension and the influencing factors that lead to PVST.
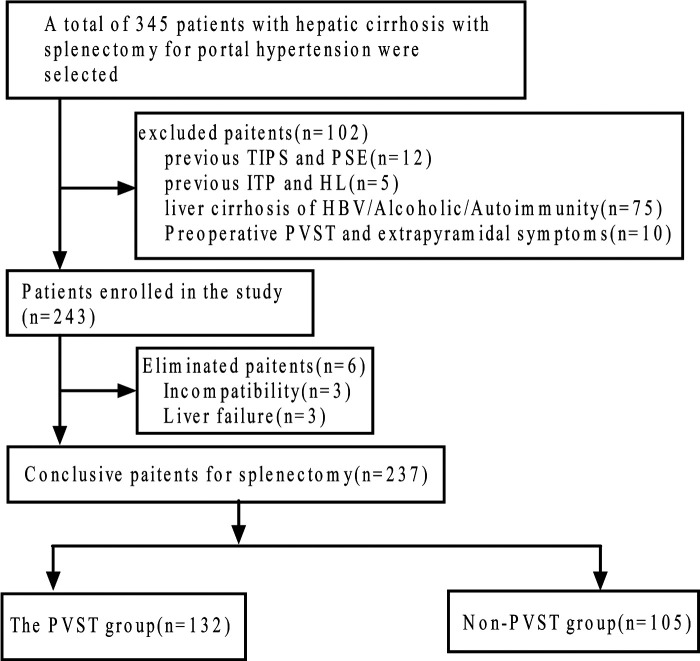
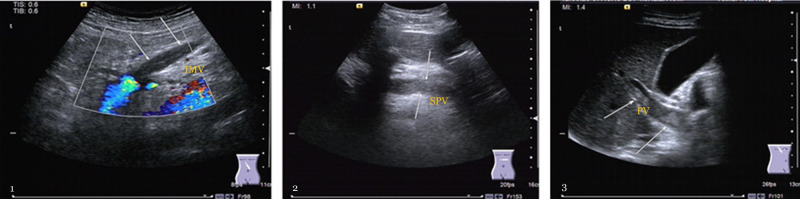
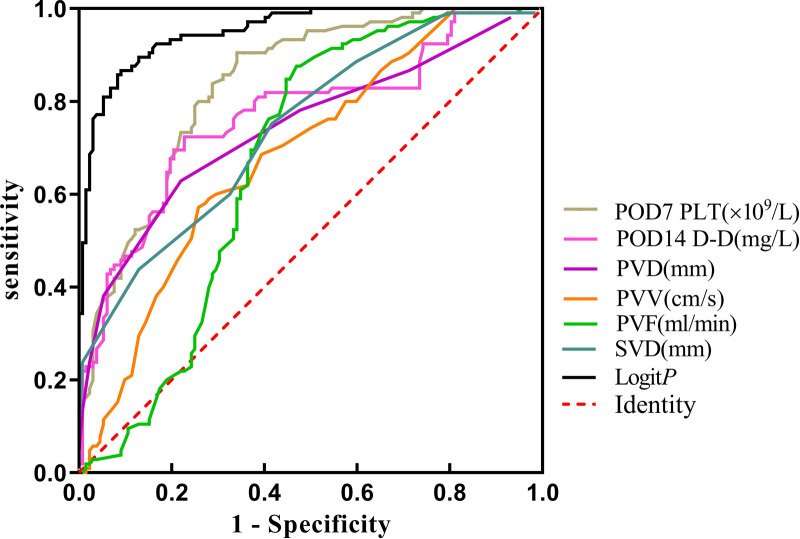
A retrospective cohort study was conducted, in which 237 Wilson's disease patients with hypersplenism underwent splenectomy. The hemodynamic indices of the portal vein were monitored before surgery and on the 1st, 7th, and 14th days around surgery. The patients were divided into PVST and non-PVST groups. The clinical factors were identified by univariate and multivariate logistic regression. The Logit was calculated according to the logistic regression prediction model, and the ROC curve for each independent factor was plotted.
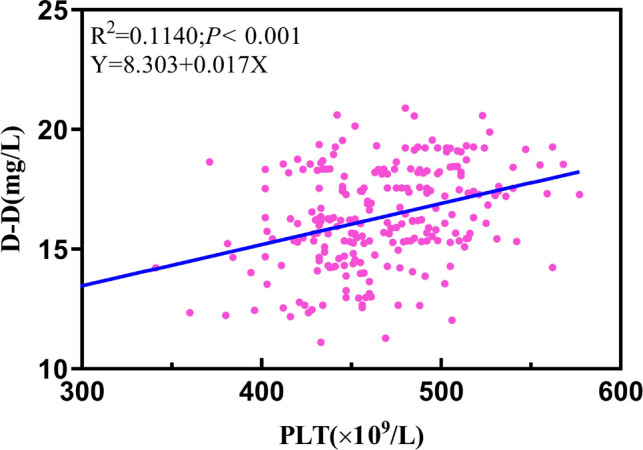
The portal vein velocity, flow, and inner diameter showed a downward trend around surgery, with statistically significant differences between each time point (< 0.01). The PVST incidence rate was 55.7%. Univariate analysis revealed that the platelet (PLT) levels on the postoperative 3rd and 7th days (= 0.001; < 0.001), D-dimer (D-D) on the postoperative 7th and 14th days (= 0.002; < 0.001), preoperative portal vein velocity, flow, diameter (< 0.001), and splenic vein diameter (< 0.001) were all statistically and significantly different between the two groups. Multivariate logistic regression revealed a significant increase in PLT on the postoperative 7th day (OR= 1.043, 95% CI, 1.027-1.060, < 0.001) and D-D on the postoperative 14th day (OR = 1.846, 95% CI, 1.400-2.435, < 0.001). Preoperative portal and splenic vein diameters (OR = 1.565, 95% CI, 1.213-2.019, = 0.001; OR = 1.671, 95% CI, 1.305-2.140, < 0.001) were the risk factors for PVST. However, preoperative portal vein velocity and flow (OR = 0.578, 95% CI, 0.409-0.818, = 0.002; OR= 0.987, 95% CI, 0.975-0.990, = 0.046) were protective factors for PVST. Logit was calculated using a logistic regression prediction model with a cut-off value of -0.32 and an area under receiver operating characteristic curve of 0.952 with 88.61% accuracy.
Splenectomy relieves portal hypertension by reducing the hemodynamics index. PVST is linked to multiple factors, including preoperative portal vein diameter, velocity, flow, and splenic vein diameter, especially PLT on the postoperative 7th day and D-D on the postoperative 14th day. The predictive model is accurate in predicting PVST.
脾切除术是门静脉高压合并脾功能亢进的关键治疗手段之一。然而,血流动力学改变引起的门静脉系统血栓形成(PVST)会影响患者预后。本研究分析肝豆状核变性合并门静脉高压患者脾切除术后门静脉血流动力学变化及导致PVST的影响因素。
进行一项回顾性队列研究,237例脾功能亢进的肝豆状核变性患者接受脾切除术。于术前及术后第1、7、14天监测门静脉血流动力学指标。将患者分为PVST组和非PVST组。通过单因素和多因素logistic回归分析确定临床因素。根据logistic回归预测模型计算Logit值,并绘制各独立因素的ROC曲线。
门静脉流速、流量及内径在手术前后呈下降趋势,各时间点差异有统计学意义(<0.01)。PVST发生率为55.7%。单因素分析显示,术后第3天和第7天的血小板(PLT)水平(=0.001;<0.001)、术后第7天和第14天的D-二聚体(D-D)(=0.002;<0.001)、术前门静脉流速、流量、内径(<0.001)及脾静脉内径(<0.001)在两组间差异均有统计学意义。多因素logistic回归显示,术后第7天PLT显著升高(OR=1.043,95%CI,1.027-1.060,<0.001),术后第14天D-D升高(OR=1.846,95%CI,1.400-2.435,<0.001)。术前门静脉及脾静脉内径(OR=1.565,95%CI,1.213-2.019,=0.001;OR=1.671,95%CI,1.305-2.140,<0.001)是PVST的危险因素。然而,术前门静脉流速和流量(OR=0.578,95%CI,0.409-0.818,=0.002;OR=0.987,95%CI,0.975-0.990,=0.046)是PVST的保护因素。使用logistic回归预测模型计算Logit值,截断值为-0.32,受试者工作特征曲线下面积为0.952,准确率为88.61%。
脾切除术通过降低血流动力学指标缓解门静脉高压。PVST与多种因素有关,包括术前门静脉内径、流速、流量及脾静脉内径,尤其是术后第7天的PLT和术后第14天的D-D。该预测模型对PVST具有较高预测准确性。