Leen N A, de Weijer A D, van Rooij S J H, Kennis M, Baas J M P, Geuze E
University Medical Center, Utrecht, the Netherlands.
Brain Research and Innovation Center, Ministry of Defence, Utrecht, the Netherlands.
Chronic Stress (Thousand Oaks). 2022 Jun 9;6:24705470221107290. doi: 10.1177/24705470221107290. eCollection 2022 Jan-Dec.
Although current treatments for Post-Traumatic Stress Disorder (PTSD) in war veterans are effective, unfortunately 30-50% still do not benefit from these treatments. Trauma-focused therapies, eg exposure therapy, are primarily based on extinction processes in which the endocannabinoid system (ECS) plays a significant role. Therefore, it can be hypothesized that poor treatment response on trauma-focused therapy due to extinction deficits may be associated with a poorly functioning ECS. The present study examined whether the endocannabinoids anandamide (AEA) and 2-arachidonylglycerol (2-AG) are associated with post-treatment symptom reduction.
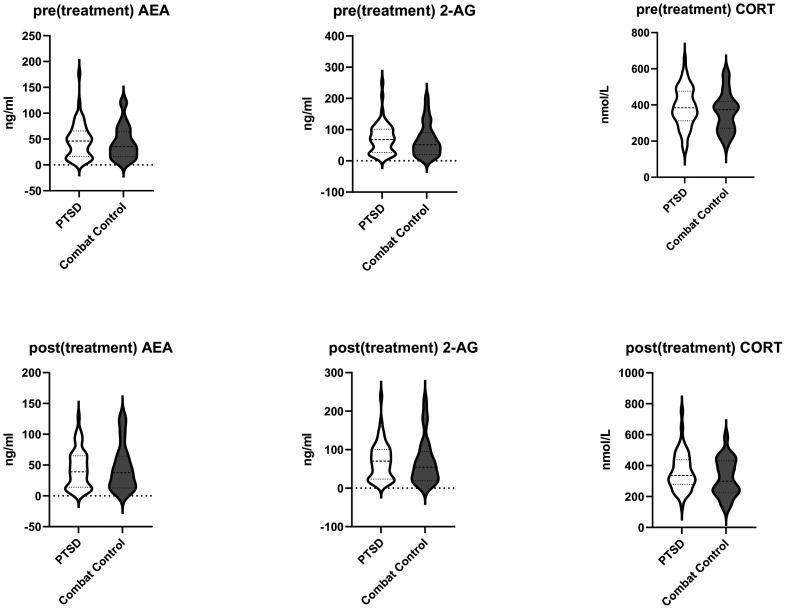
Blood plasma levels of AEA and 2-AG were determined in war veterans with a PTSD diagnosis ( = 54) and combat controls ( = 26) before and after a 6-8 month interval. During this period veterans with PTSD received trauma-focused therapy (eg cognitive behavioral therapy with exposure or eye-movement desensitization and reprocessing). Clinical symptoms were assessed before and after therapy with the Clinician Administered PTSD Scale (CAPS), State-Trait Anxiety Inventory (STAI) and Mood and Anxiety Symptom Questionnaire (MASQ).
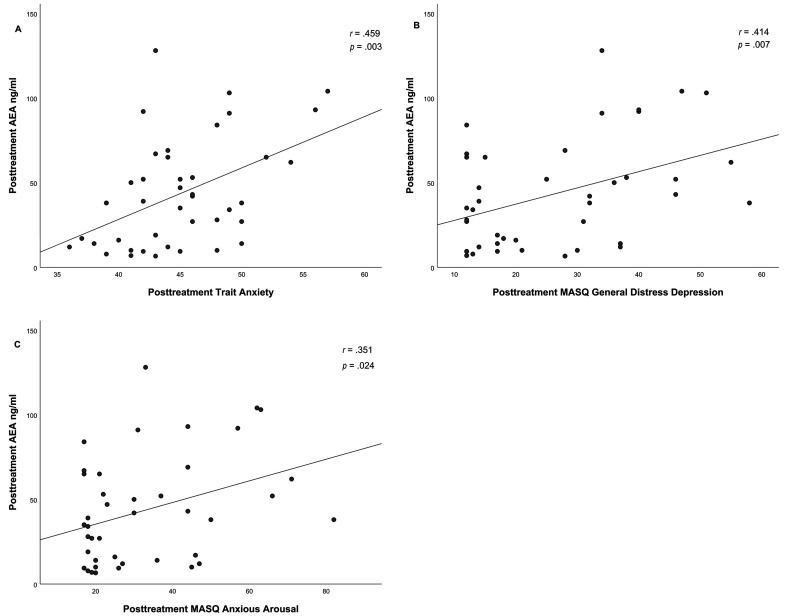
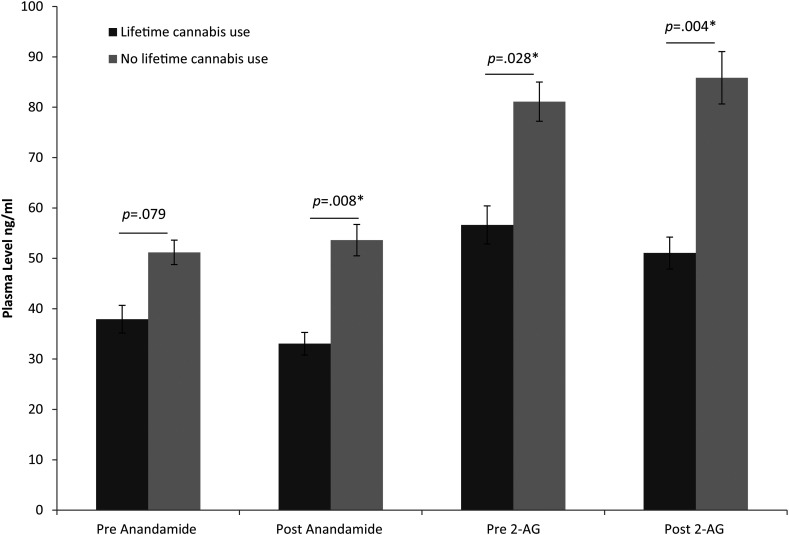
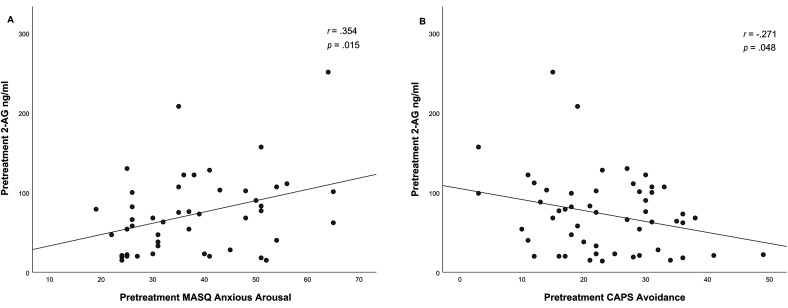
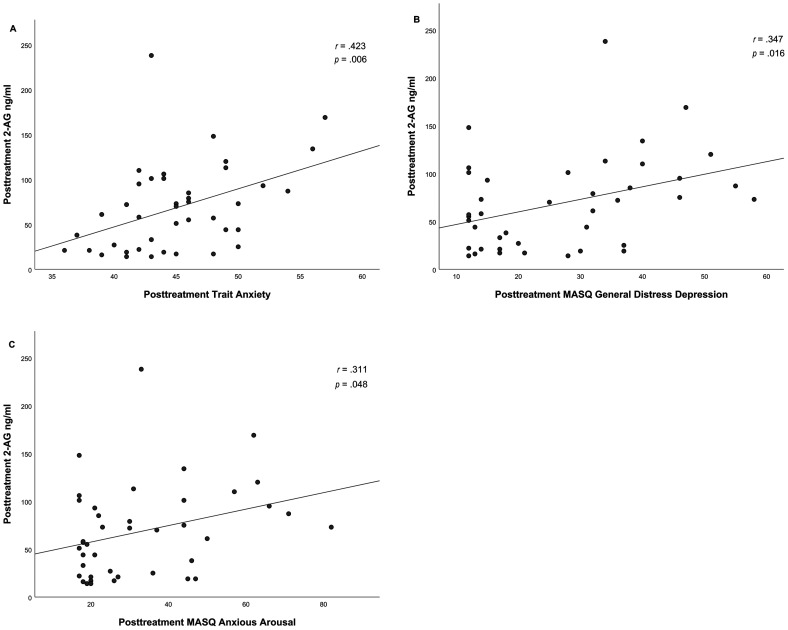
Regression analysis demonstrated that pretreatment endocannabinoid levels were not predictive of PTSD symptom reduction. Additionally, baseline endocannabinoid levels did not differ between either PTSD and combat controls or between combat controls, treatment responders, and non-responders. Only cortisol levels significantly decreased over time from pre- to posttreatment ( = .041). Endocannabinoid levels were significantly lower in individuals who reported cannabis use during their lifetime, independent of PTSD diagnosis. Furthermore, correlation analysis revealed that pretreatment 2-AG levels in PTSD were positively correlated with anxious arousal ( .354, = .015) and negatively with avoidance symptoms ( .271, = .048). Both posttreatment AEA and 2-AG were positively correlated with trait anxiety (AEA .459, = .003; 2-AG .423, = .006), anxious arousal (AEA .351, = .024; 2-AG .311, = .048) and general distress depression symptoms (AEA .414, = .007; 2-AG .374, = .016).
Since endocannabinoids are mainly generated 'on demand', future work could benefit by investigating endocannabinoid circulation under both baseline and stressful conditions. In line with previous research cannabis use was associated with lower endocannabinoid levels. The correlation analysis between pre- and posttreatment endocannabinoid levels and pre- and posttreatment clinical symptomatology were exploratory analysis and should be replicated in future research.
尽管目前针对退伍军人创伤后应激障碍(PTSD)的治疗方法有效,但不幸的是,仍有30 - 50%的患者无法从这些治疗中获益。以创伤为重点的疗法,如暴露疗法,主要基于消退过程,其中内源性大麻素系统(ECS)起着重要作用。因此,可以假设,由于消退缺陷导致的以创伤为重点的治疗反应不佳可能与ECS功能不良有关。本研究调查了内源性大麻素花生四烯乙醇胺(AEA)和2 - 花生四烯酸甘油(2 - AG)是否与治疗后症状减轻有关。
在6 - 8个月的间隔前后,测定了54名被诊断为PTSD的退伍军人和26名战斗对照者的血浆AEA和2 - AG水平。在此期间,患有PTSD的退伍军人接受了以创伤为重点的治疗(如认知行为疗法与暴露疗法或眼动脱敏再处理疗法)。治疗前后用临床医生评定的PTSD量表(CAPS)、状态 - 特质焦虑量表(STAI)和情绪与焦虑症状问卷(MASQ)评估临床症状。
回归分析表明,治疗前内源性大麻素水平不能预测PTSD症状的减轻。此外,PTSD患者与战斗对照者之间,或战斗对照者、治疗反应者和无反应者之间的基线内源性大麻素水平没有差异。只有皮质醇水平从治疗前到治疗后随时间显著降低(P = 0.041)。报告一生中使用过大麻的个体,其体内内源性大麻素水平显著较低,与PTSD诊断无关。此外,相关分析显示,PTSD患者治疗前的2 - AG水平与焦虑唤醒呈正相关(r = 0.354,P = 0.015),与回避症状呈负相关(r = - 0.271,P = 0.048)。治疗后的AEA和2 - AG均与特质焦虑呈正相关(AEA:r = 0.459,P = 0.003;2 - AG:r = 0.423,P = 0.006),与焦虑唤醒呈正相关(AEA:r = 0.351,P = 0.024;2 - AG:r = 0.311,P = 0.048),与一般痛苦抑郁症状呈正相关(AEA:r = 0.414,P = 0.007;2 - AG:r = 0.374,P = 0.016)。
由于内源性大麻素主要是“按需”产生的,未来的研究可以通过调查基线和应激条件下的内源性大麻素循环而受益。与先前的研究一致,大麻使用与较低的内源性大麻素水平相关。治疗前后内源性大麻素水平与治疗前后临床症状学之间的相关分析是探索性分析,应在未来的研究中重复进行。