Pharmaceutical Analysis Research Group, Groningen Research Institute of Pharmacy, University of Groningen, Antonius Deusinglaan 1, 9713 AV, Groningen, The Netherlands.
Analytical Biochemistry Research Group, Groningen Research Institute of Pharmacy, University of Groningen, A. Deusinglaan 16, 9713 AV, Groningen, The Netherlands.
Arch Toxicol. 2022 Sep;96(9):2523-2543. doi: 10.1007/s00204-022-03321-2. Epub 2022 Jun 16.
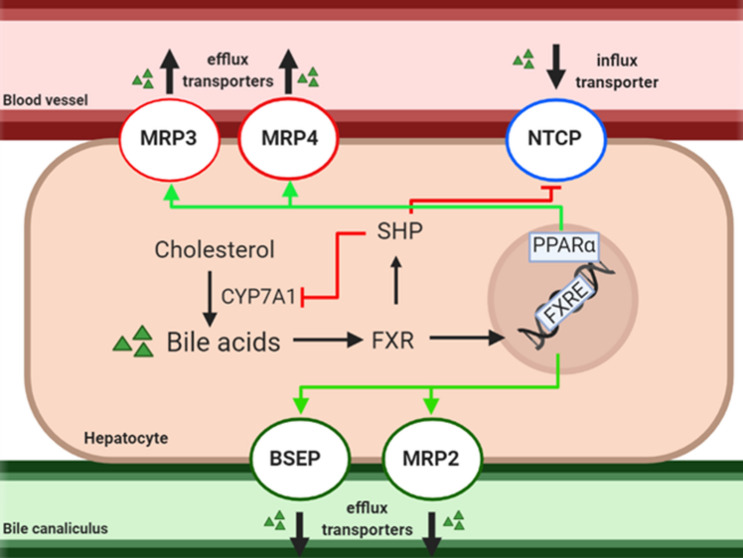
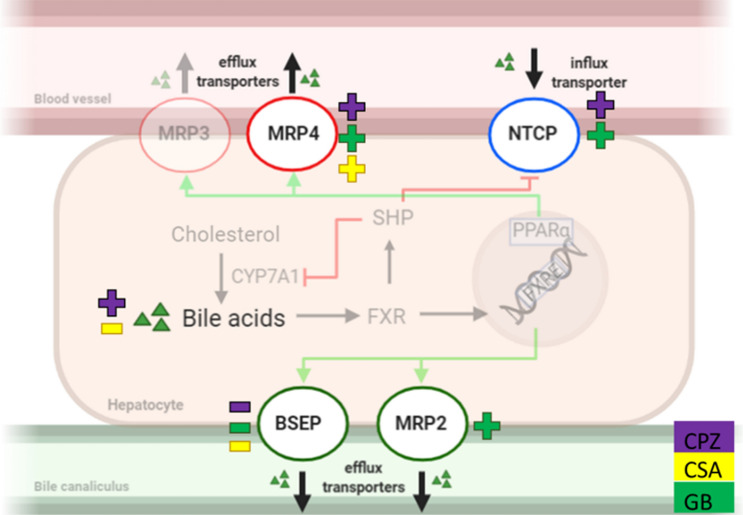
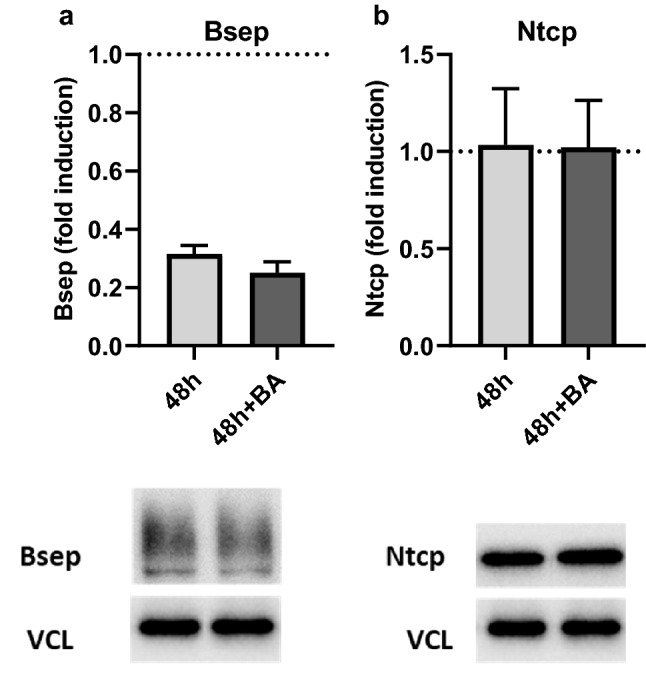
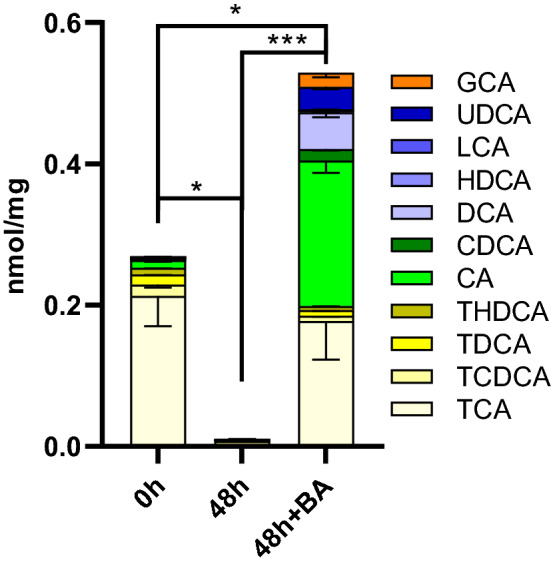
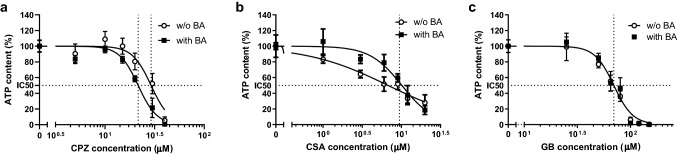
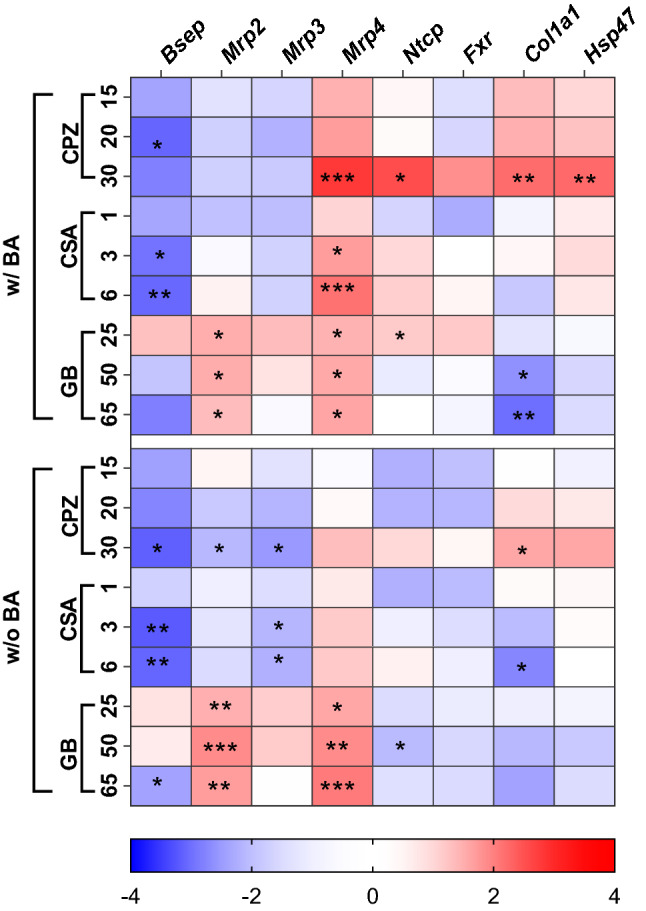
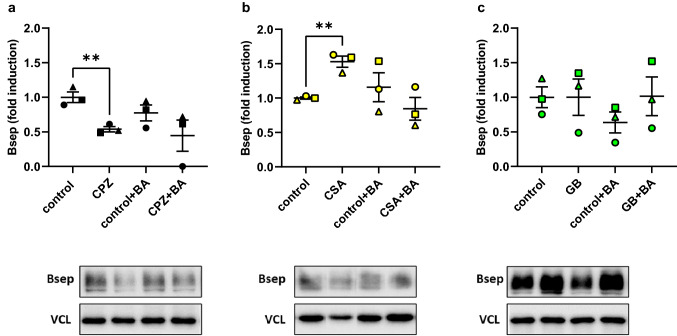
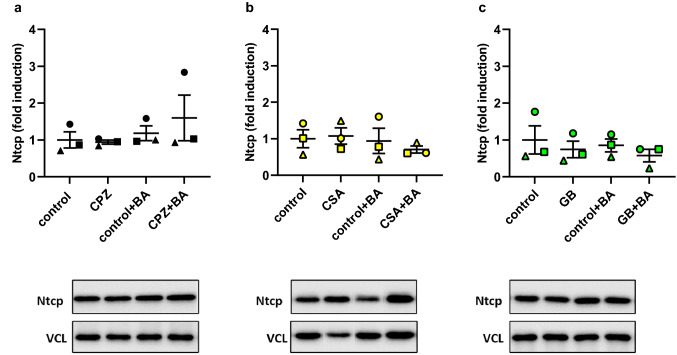
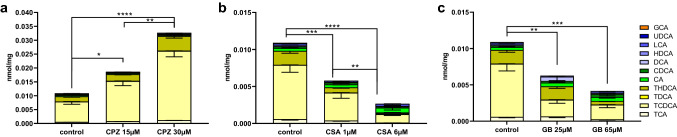
Drugs are often withdrawn from the market due to the manifestation of drug-induced liver injury (DILI) in patients. Drug-induced cholestasis (DIC), defined as obstruction of hepatic bile flow due to medication, is one form of DILI. Because DILI is idiosyncratic, and the resulting cholestasis complex, there is no suitable in vitro model for early DIC detection during drug development. Our goal was to develop a mouse precision-cut liver slice (mPCLS) model to study DIC and to assess cholestasis development using conventional molecular biology and analytical chemistry methods. Cholestasis was induced in mPCLS through a 48-h-incubation with three drugs known to induce cholestasis in humans, namely chlorpromazine (15, 20, and 30 µM), cyclosporin A (1, 3, and 6 µM) or glibenclamide (25, 50, and 65 µM). A bile-acid mixture (16 µM) that is physiologically representative of the human bile-acid pool was added to the incubation medium with drug, and results were compared to incubations with no added bile acids. Treatment of PCLS with cholestatic drugs increased the intracellular bile-acid concentration of deoxycholic acid and modulated bile-transporter genes. Chlorpromazine led to the most pronounced cholestasis in 48 h, observed as increased toxicity; decreased protein and gene expression of the bile salt export pump; increased gene expression of multidrug resistance-associated protein 4; and accumulation of intracellular bile acids. Moreover, chlorpromazine-induced cholestasis exhibited some transition into fibrosis, evidenced by increased gene expression of collagen 1A1 and heatshock protein 47. In conclusion, we demonstrate that mPCLS can be used to study human DIC onset and progression in a 48 h period. We thus propose this model is suited for other similar studies of human DIC.
由于患者出现药物性肝损伤 (DILI),药物经常从市场上撤出。药物性胆汁淤积症 (DIC),定义为药物引起的肝内胆汁流动受阻,是 DILI 的一种形式。由于 DILI 是体质特异的,并且由此产生的胆汁淤积复杂,因此在药物开发过程中没有合适的体外模型来早期检测 DIC。我们的目标是开发一种小鼠精密切割肝切片 (mPCLS) 模型来研究 DIC,并使用常规分子生物学和分析化学方法评估胆汁淤积的发展。通过在 mPCLS 中孵育 48 小时来诱导胆汁淤积,孵育物中含有三种已知会引起人类胆汁淤积的药物,即氯丙嗪(15、20 和 30 μM)、环孢素 A(1、3 和 6 μM)或格列本脲(25、50 和 65 μM)。孵育物中添加了生理上代表人类胆汁酸池的混合胆汁酸(16 μM),并将结果与未添加胆汁酸的孵育物进行了比较。用胆汁淤积药物处理 PCLS 会增加脱氧胆酸的细胞内胆汁酸浓度并调节胆汁转运蛋白基因。氯丙嗪在 48 小时内导致最明显的胆汁淤积,表现为毒性增加;胆汁盐输出泵的蛋白和基因表达降低;多药耐药相关蛋白 4 的基因表达增加;以及细胞内胆汁酸的积累。此外,氯丙嗪诱导的胆汁淤积表现出一些向纤维化的转变,这表现为胶原蛋白 1A1 和热休克蛋白 47 的基因表达增加。总之,我们证明 mPCLS 可用于在 48 小时内研究人类 DIC 的发病和进展。因此,我们建议该模型适用于其他类似的人类 DIC 研究。