Chinese People's Liberation Army (PLA) Medical School, Beijing, China.
Department of Infectious Diseases, The Fifth Medical Center of Chinese People's Liberation Army (PLA) General Hospital, Beijing, China.
Front Immunol. 2022 May 25;13:892618. doi: 10.3389/fimmu.2022.892618. eCollection 2022.
Thus far, few studies have investigated the safety and efficacy of programmed death-1 (PD-1) immune checkpoint inhibitors (ICIs) and tyrosine kinase inhibitors (TKIs) antibodies in patients with hepatitis B virus (HBV)-related liver cancer.
To investigate the effect of combination therapy with programmed death-1 (PD-1) immune checkpoint inhibitors (ICIs) and tyrosine kinase inhibitors (TKIs) on HBV-related liver cancer.
Until January 31, 2022, liver cancer patients with hepatitis B surface antigen (HBsAg) or HBV DNA positivity, treated with PD-1 ICIs and TKIs combined with nucleoside analogs (NAs), were retrospectively reviewed. The correlation between the change in HBV DNA and HBsAg levels and tumor response was analyzed using the χ test. Cox univariate and multivariate survival analyses and Kaplan-Meier curves were used to identify and compare risk factors and overall survival (OS).
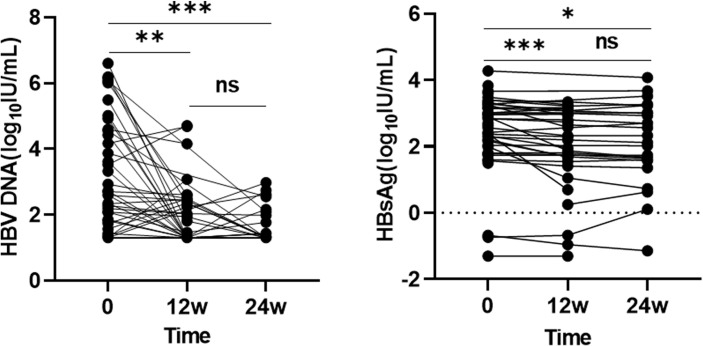
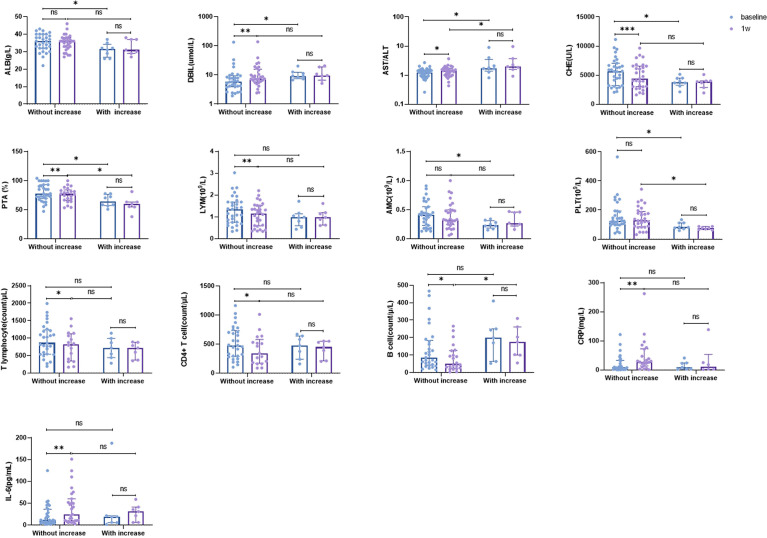
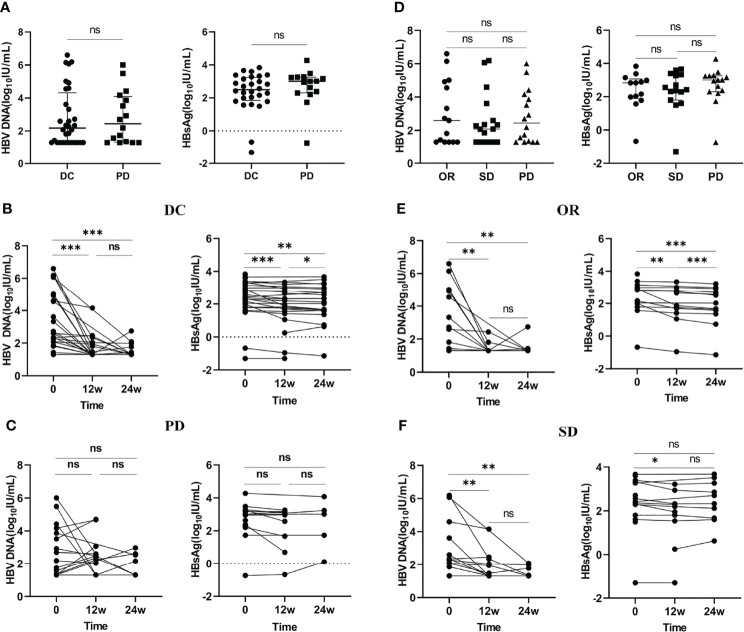
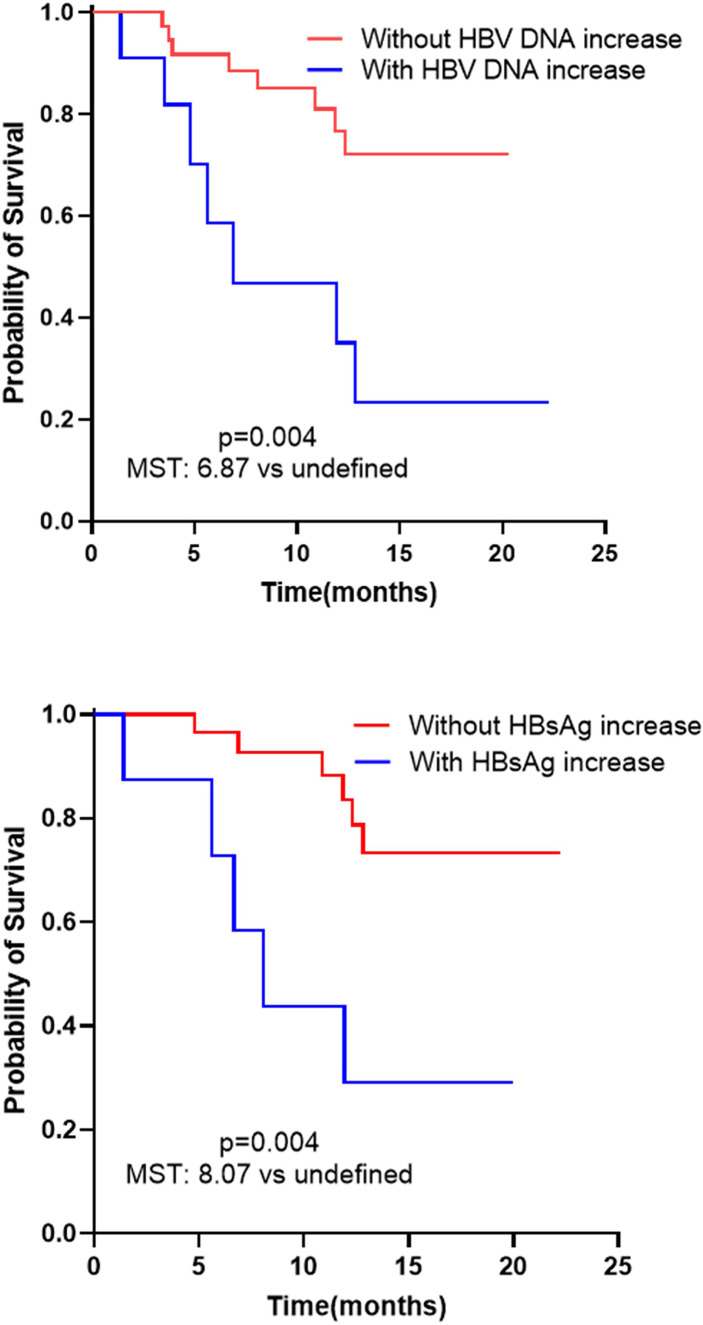
A total of 48 patients were enrolled in the study, with an objective response rate (ORR) of 31.3%, a disease control rate (DCR) of 66.7%; the incidence of adverse events was mostly mild. A significant decrease in HBV DNA and HBsAg levels was observed at 12 and 24 weeks compared with the baseline (p < 0.05). Compared to patients with progressive disease (PD), patients with disease control showed a more significant decrease in HBV DNA and HBsAg levels at 12 and 24 weeks (p < 0.001). Eleven patients showed elevations in HBV DNA level and one of them showed HBV reactivation; however, the reactivation was not associated hepatitis. Moreover, eight patients showed elevation in HBsAg. Elevation in HBV DNA level was associated with poor tumor response (P=0.001, OR=18.643 [95% CI: 3.271-106.253]). Cox survival analysis suggested that HBV DNA increase (P=0.011, HR=4.816, 95% CI: 1.439-16.117) and HBsAg increase (P=0.022, HR=4.161, 95% CI: 1.224-16.144) were independent risk factors associated with survival time. Kaplan-Meier curves suggested that patients who exhibited an increase in HBV DNA (6.87 months undefined, log-rank test: p= 0.004) and HBsAg (8.07 months undefined, log-rank test: p= 0.004) levels had a shorter median survival time (MST). Patients without increased HBsAg showed better baseline liver function and routine blood tests (p<0.05) than patients with increased HBsAg. An increase in C-reactive protein (CRP) and interleukin-6 (IL-6), and a decrease in T lymphocytes, CD4+ T lymphocytes, and B lymphocytes at 1-week post-treatment associated with HBsAg well-controlled.
HBV-related liver cancer patients treated with combination therapy showed improved efficacy and safety profiles. Combination therapy has some effect on HBV infection, and a correlation between tumor response and antiviral efficacy was found. Elevation of HBV DNA and HBsAg levels may indicate poorer tumor response and survival time. Better baseline liver function and early immune activation may be associated with decline in HBsAg levels.
迄今为止,鲜有研究探讨程序性死亡-1(PD-1)免疫检查点抑制剂(ICIs)和酪氨酸激酶抑制剂(TKIs)抗体在乙型肝炎病毒(HBV)相关肝癌患者中的安全性和疗效。
探讨 PD-1 免疫检查点抑制剂(ICIs)和酪氨酸激酶抑制剂(TKIs)联合治疗对 HBV 相关肝癌的疗效。
截至 2022 年 1 月 31 日,回顾性分析了乙型肝炎表面抗原(HBsAg)或 HBV DNA 阳性、接受 PD-1 ICIs 和 TKI 联合核苷类似物(NAs)治疗的肝癌患者。采用卡方检验分析 HBV DNA 和 HBsAg 水平变化与肿瘤反应的相关性。Cox 单因素和多因素生存分析和 Kaplan-Meier 曲线用于确定和比较风险因素和总生存期(OS)。
共纳入 48 例患者,客观缓解率(ORR)为 31.3%,疾病控制率(DCR)为 66.7%;不良事件发生率多为轻度。与基线相比,在 12 和 24 周时观察到 HBV DNA 和 HBsAg 水平显著下降(p<0.05)。与疾病进展(PD)患者相比,疾病控制患者在 12 和 24 周时 HBV DNA 和 HBsAg 水平下降更为显著(p<0.001)。11 例患者 HBV DNA 水平升高,其中 1 例出现 HBV 再激活;然而,再激活与肝炎无关。此外,8 例患者 HBsAg 升高。HBV DNA 水平升高与肿瘤反应不良相关(P=0.001,OR=18.643 [95%CI:3.271-106.253])。Cox 生存分析提示 HBV DNA 升高(P=0.011,HR=4.816,95%CI:1.439-16.117)和 HBsAg 升高(P=0.022,HR=4.161,95%CI:1.224-16.144)是与生存时间相关的独立危险因素。Kaplan-Meier 曲线提示 HBV DNA 升高(6.87 个月 未定义,log-rank 检验:p=0.004)和 HBsAg 升高(8.07 个月 未定义,log-rank 检验:p=0.004)的患者中位生存时间(MST)更短。与 HBsAg 升高的患者相比,HBsAg 未升高的患者基线肝功能和常规血液检查更好(p<0.05)。治疗后 1 周时 C-反应蛋白(CRP)和白细胞介素-6(IL-6)升高以及 T 淋巴细胞、CD4+T 淋巴细胞和 B 淋巴细胞减少与 HBsAg 控制良好相关。
接受联合治疗的 HBV 相关肝癌患者显示出改善的疗效和安全性特征。联合治疗对 HBV 感染具有一定疗效,并且发现肿瘤反应与抗病毒疗效之间存在相关性。HBV DNA 和 HBsAg 水平升高可能预示着肿瘤反应和生存时间较差。更好的基线肝功能和早期免疫激活可能与 HBsAg 水平下降有关。