Yuan Guosheng, Li Rong, Li Qi, Hu Xiaoyun, Ruan Jian, Fan Wenzhe, Wang Junjie, Huang Wei, Zang Mengya, Chen Jinzhang
Department of Infectious Diseases and Hepatology Unit, Nanfang Hospital, Southern Medical University, Guangzhou, China.
Department of Medical Oncology, The First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, China.
Ann Transl Med. 2021 Sep;9(18):1412. doi: 10.21037/atm-21-3020.
The interaction between hepatitis B virus (HBV) load and anti-programmed cell death (PD)-1 in combination with (+) antiangiogenic therapy remains controversial, especially for hepatocellular carcinoma (HCC) patients. This study sought to explore the effects of HBV load and antiviral therapy on anti-PD-1+ antiangiogenic therapy, and the rate of HBV reactivation during anti-PD-1+ antiangiogenic treatment.
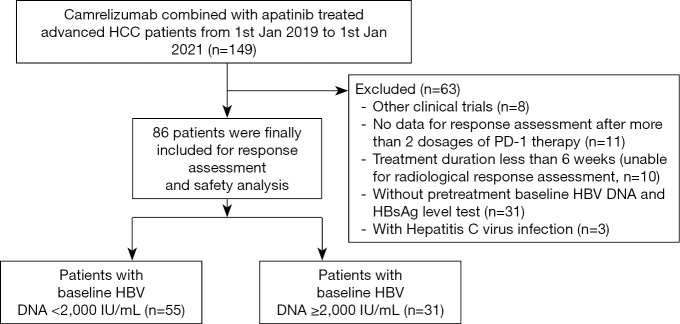
We performed a multicenter retrospective cohort study of camrelizumab combined with apatinib (C+A) therapy between January 1, 2019 and January 1, 2021 in patients with unresectable HCC who were seropositive for hepatitis B surface antigen (HBsAg) and received antiviral therapy before C+A involvement. The effects of HBV load and antiviral therapy on C+A and the rate of HBV reactivation during C+A treatment were examined.
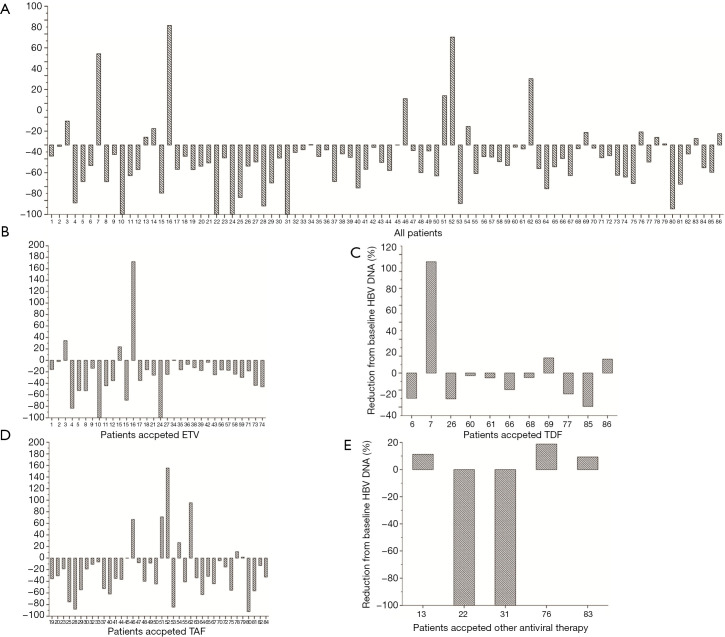
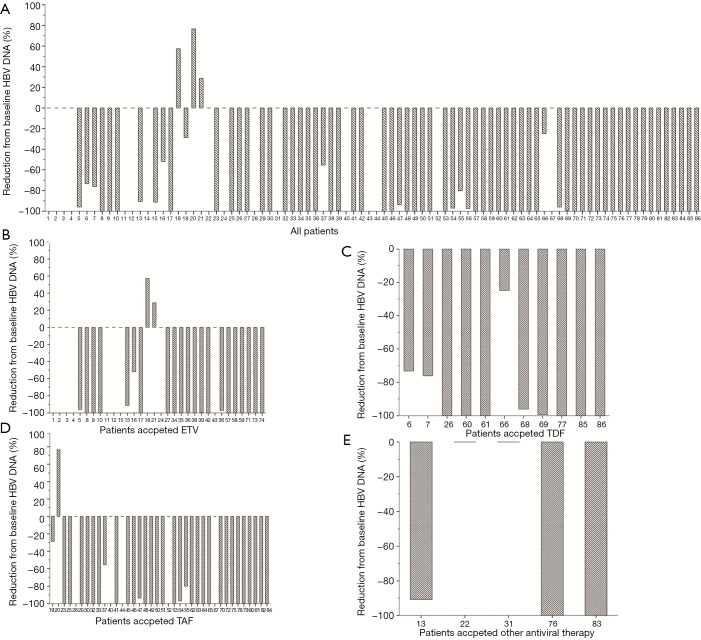
Eighty-six patients were included in the analysis. The patients had a mean age of 55 years, and 72 (83.7%) were male. The objective response rates (ORRs) in patients with low (<2,000 IU/mL) and high (≥2,000 IU/mL) baseline HBV deoxyribonucleic acid (DNA) levels were 34.5% and 32.2%, respectively (χ=0.046; P=0.829), while the disease control rates (DCRs) were 67.3% and 80.6%, respectively (χ=1.762; P=0.184). The results of the univariate and multivariate analyses showed that the baseline HBV DNA level did not affect PD. Additionally, none of the 86 patients suffered from HBV reactivation or HBV-related hepatic impairment with continuous antiviral treatment, regardless of nucleos(t)ide analogue (NA) type (F=1.473; P=0.228).
Baseline HBV loads did not affect the tumor responses of HCC patients receiving anti-PD-1+ antiangiogenic therapy. Thus, HBV reactivation should not be a contradiction for anti-PD-1+ antiangiogenic therapy among patients undergoing continuous and effective antiviral treatment.
乙型肝炎病毒(HBV)载量与抗程序性细胞死亡(PD)-1联合(+)抗血管生成治疗之间的相互作用仍存在争议,尤其是对于肝细胞癌(HCC)患者。本研究旨在探讨HBV载量和抗病毒治疗对抗PD-1+抗血管生成治疗的影响,以及抗PD-1+抗血管生成治疗期间HBV再激活率。
我们对2019年1月1日至2021年1月1日期间接受卡瑞利珠单抗联合阿帕替尼(C+A)治疗的不可切除HCC患者进行了一项多中心回顾性队列研究,这些患者乙肝表面抗原(HBsAg)血清学阳性,且在接受C+A治疗前接受了抗病毒治疗。研究了HBV载量和抗病毒治疗对C+A的影响以及C+A治疗期间HBV再激活率。
86例患者纳入分析。患者的平均年龄为55岁,72例(83.7%)为男性。基线HBV脱氧核糖核酸(DNA)水平低(<2000 IU/mL)和高(≥2000 IU/mL)的患者的客观缓解率(ORR)分别为34.5%和32.2%(χ=0.046;P=0.829),而疾病控制率(DCR)分别为67.3%和80.6%(χ=1.762;P=0.184)。单因素和多因素分析结果显示,基线HBV DNA水平不影响PD。此外,86例患者中无一例因持续抗病毒治疗而发生HBV再激活或HBV相关肝损伤,无论核苷(酸)类似物(NA)类型如何(F=1.473;P=0.228)。
基线HBV载量不影响接受抗PD-1+抗血管生成治疗的HCC患者的肿瘤反应。因此,对于接受持续有效抗病毒治疗的患者,HBV再激活不应成为抗PD-1+抗血管生成治疗的禁忌。