Sun Xuqi, Hu Dandan, Yang Zhoutian, Liu Zheng, Wang Juncheng, Chen Jinbin, Xu Li, Zhou Zhongguo, Chen Minshan, Zhang Yaojun
Sun Yat-Sen University Cancer Center, State Key Laboratory of Oncology in South China; Collaborative Innovation Center for Cancer Medicine, Guangzhou 510060, People's Republic of China.
Department of Liver Surgery, Sun Yat-Sen University Cancer Center, Guangzhou 510060, People's Republic of China.
J Hepatocell Carcinoma. 2020 Dec 1;7:337-345. doi: 10.2147/JHC.S278527. eCollection 2020.
A high hepatitis B virus (HBV) load is a common exclusion criterion in hepatocellular carcinoma (HCC) clinical trials for anti-programmed cell death (PD)-1 immunotherapy. However, the validity of this criterion is barely verified. This study aimed to evaluate the impact of baseline HBV DNA levels and antiviral therapy on the oncological outcomes and liver functions of patients with HCC receiving anti-PD-1 immunotherapy.
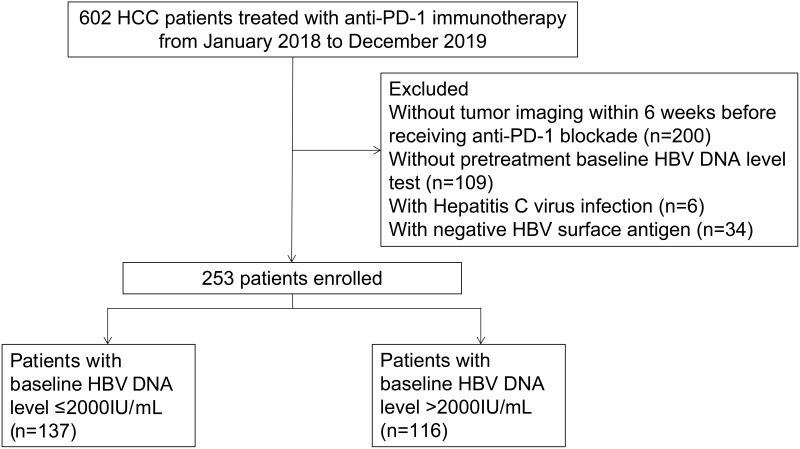
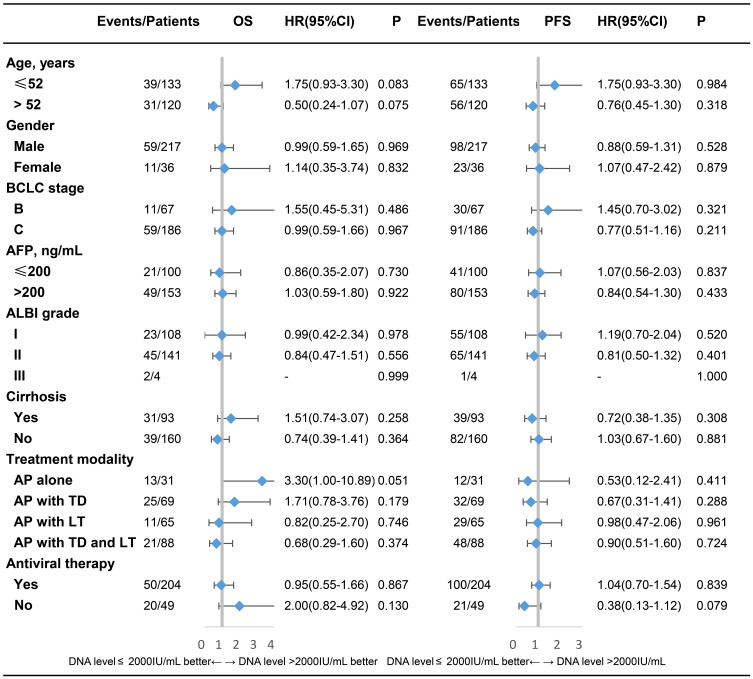
We reviewed HCC trials related to anti-PD-(L)1 immunotherapy and whether they ruled out patients with increased HBV loads on clinicaltrials.gov. Then, for this retrospective study, we enrolled 253 HCC patients treated with anti-PD-1 blockade in our institution. Baseline information was compared between patients with low and high HBV loads. Overall survival (OS) and progression-free survival (PFS) were compared, and univariate and multivariate analyses were applied to identify potential risk factors for oncological outcomes and hepatic impairment.
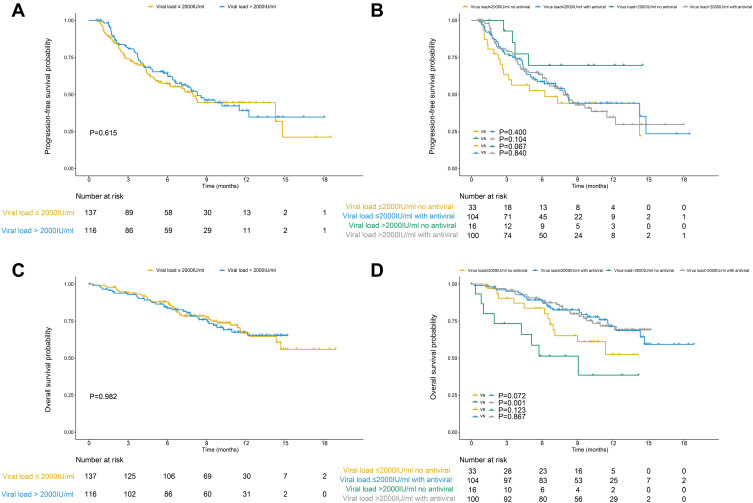
Among 76 HCC clinical trials including 13,927 patients receiving anti-PD-(L)1 blockade, 41 (53.9%) excluded patients with relatively high baseline HBV loads. The PFS and OS did not differ significantly between patients with baseline HBV loads ≤ 2000 IU/mL and those with viral loads >2000 IU/mL (p=0.615 and 0.982). The incidence of hepatic impairment showed no association with the baseline HBV load (p=0.319). Patients receiving antiviral therapy had a better OS than those without antiviral therapy in the high baseline HBV load group (p= 0.001).
High HBV loads did not compromise the clinical outcomes of HCC patients receiving anti-PD-1 blockade. Antiviral therapy could improve the OS of HCC patients with high HBV loads.
高乙肝病毒(HBV)载量是肝细胞癌(HCC)抗程序性细胞死亡(PD)-1免疫治疗临床试验中常见的排除标准。然而,该标准的有效性几乎未得到验证。本研究旨在评估基线HBV DNA水平和抗病毒治疗对接受抗PD-1免疫治疗的HCC患者肿瘤学结局和肝功能的影响。
我们在clinicaltrials.gov上检索了与抗PD-(L)1免疫治疗相关的HCC试验,以及它们是否排除了HBV载量升高的患者。然后,对于这项回顾性研究,我们纳入了在我们机构接受抗PD-1阻断治疗的253例HCC患者。比较了低HBV载量和高HBV载量患者的基线信息。比较了总生存期(OS)和无进展生存期(PFS),并进行单因素和多因素分析以确定肿瘤学结局和肝损伤的潜在危险因素。
在76项HCC临床试验中,包括13927例接受抗PD-(L)1阻断治疗的患者,41项(53.9%)排除了基线HBV载量相对较高的患者。基线HBV载量≤2000 IU/mL的患者与病毒载量>2000 IU/mL的患者之间的PFS和OS无显著差异(p=0.615和0.982)。肝损伤的发生率与基线HBV载量无关(p=0.319)。在高基线HBV载量组中,接受抗病毒治疗的患者比未接受抗病毒治疗的患者OS更好(p=0.001)。
高HBV载量并未损害接受抗PD-1阻断治疗的HCC患者的临床结局。抗病毒治疗可改善高HBV载量HCC患者的OS。