Kidney Center, Turku University Hospital and University of Turku, Turku, Finland.
Department of Anaesthesiology and Intensive Care, University of Turku, Turku, Finland.
Sci Rep. 2022 Jun 17;12(1):10177. doi: 10.1038/s41598-022-14497-z.
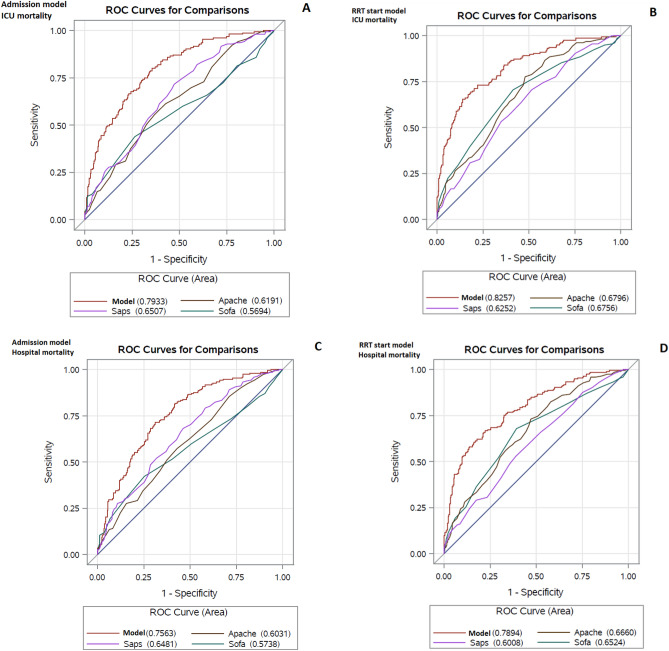
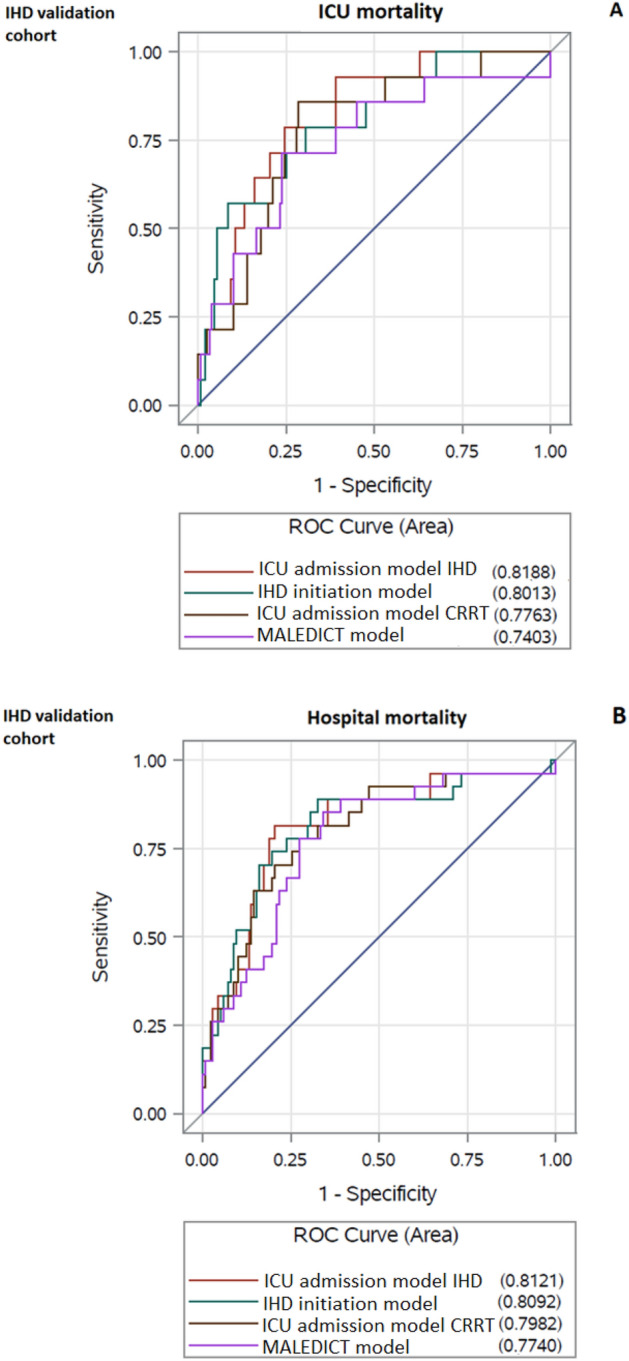
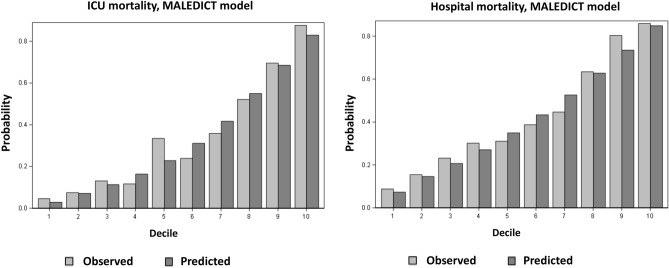
Half of the critically ill patients with renal replacement therapy (RRT) dependent acute kidney injury (AKI) die within one year despite RRT. General intensive care prediction models perform inadequately in AKI. Predictive models for mortality would be an invaluable complementary tool to aid clinical decision making. We aimed to develop and validate new prediction models for intensive care unit (ICU) and hospital mortality customized for patients with RRT dependent AKI in a retrospective single-center study. The models were first developed in a cohort of 471 critically ill patients with continuous RRT (CRRT) and then validated in a cohort of 193 critically ill patients with intermittent hemodialysis (IHD) as the primary modality for RRT. Forty-two risk factors for mortality were examined at ICU admission and CRRT initiation, respectively, in the first univariate models followed by multivariable model development. Receiver operating characteristics curve analyses were conducted to estimate the area under the curve (AUC), to measure discriminative capacity of the models for mortality. AUCs of the respective models ranged between 0.76 and 0.83 in the CRRT model development cohort, thereby showing acceptable to excellent predictive power for the mortality events (ICU mortality and hospital mortality). The models showed acceptable external validity in a validation cohort of IHD patients. In the IHD validation cohort the AUCs of the MALEDICT RRT initiation model were 0.74 and 0.77 for ICU and hospital mortality, respectively. The MALEDICT model shows promise for mortality prediction in critically ill patients with RRT dependent AKI. After further validation, the model might serve as an additional clinical tool for estimating individual mortality risk at the time of RRT initiation.
尽管接受肾脏替代治疗(RRT)的危重病患者中,有一半的急性肾损伤(AKI)患者在一年内死亡,但一般的重症监护预测模型在 AKI 中的表现并不理想。死亡率预测模型将是一种非常宝贵的辅助临床决策工具。我们旨在开发和验证新的预测模型,以评估接受 RRT 的 AKI 患者的重症监护病房(ICU)和医院死亡率,这是一项回顾性单中心研究。这些模型首先在一组 471 名接受连续肾脏替代治疗(CRRT)的危重病患者中进行开发,然后在一组 193 名接受间歇性血液透析(IHD)作为 RRT 主要方式的危重病患者中进行验证。在第一个单变量模型中,分别在 ICU 入院和 CRRT 开始时检查了 42 个与死亡率相关的风险因素,然后进行多变量模型开发。接收者操作特征曲线分析用于估计曲线下面积(AUC),以衡量模型对死亡率的区分能力。在 CRRT 模型开发队列中,各自模型的 AUC 范围在 0.76 至 0.83 之间,表明对死亡率事件(ICU 死亡率和医院死亡率)具有可接受至优异的预测能力。这些模型在 IHD 患者的验证队列中表现出可接受的外部有效性。在 IHD 验证队列中,MALEDICT RRT 起始模型的 AUC 分别为 ICU 死亡率和医院死亡率的 0.74 和 0.77。MALEDICT 模型有望预测接受 RRT 的 AKI 危重病患者的死亡率。经过进一步验证后,该模型可能成为 RRT 起始时评估个体死亡率风险的附加临床工具。