Ali Liaquat, Alhatou Mohammed, Adeli Gholam, Elalamy Osama, Zada Yasin, Mohammed Imran, Sharif Muhammad, Noor Illahi Memon, Naeem Muhammad, Iqrar Ambreen
Neurology, Hamad General Hospital, Doha, QAT.
Neurology, Weill Cornell Medicine-Qatar, Doha, QAT.
Cureus. 2022 May 16;14(5):e25047. doi: 10.7759/cureus.25047. eCollection 2022 May.
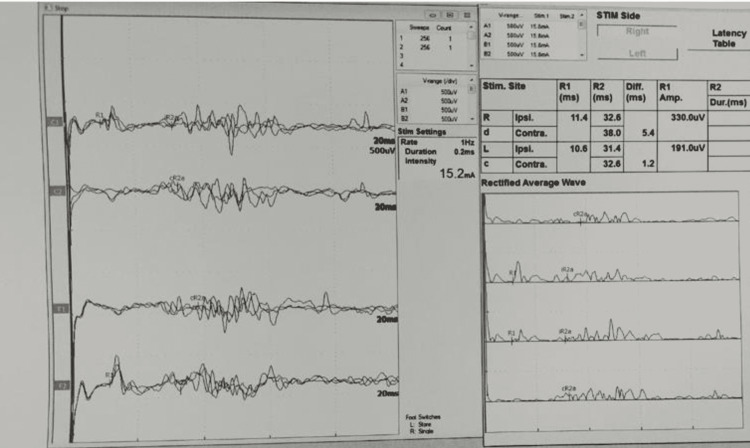
Background The etiology of facial nerve palsy is diverse and includes herpes zoster virus, Guillain-Barre syndrome (GBS), otitis media, Lyme disease, sarcoidosis, human immunodeficiency virus, etc. The lower motor neuron type facial nerve palsy is usually caused by an ipsilateral facial nerve lesion; however, it may be caused by a central lesion of the facial nerve nucleus and tract in the pons. Facial diplegia is an extremely rare condition that occurs in approximately 0.3% to 2.0% of all facial palsies. Electrodiagnostic studies including direct facial nerve conduction, facial electromyography (EMG), and blink reflex studies are useful for the prognosis and lesion localization in facial nerve palsy. Methodology This retrospective, observational study was conducted at the Neurophysiology Unit, Hamad General Hospital, Doha, Qatar. This study included 11 patients with bilateral facial weakness who visited for electrodiagnostic studies in the neurophysiology laboratory. Results In total, eight (72.7%) patients had facial diplegia, eight (72.7%) had hypo/areflexia, seven (63.6%) had facial numbness, and five (45.5%) had cerebrospinal fluid albuminocytological dissociation. The most frequent cause of facial diplegia in this study was GBS (81.9%). Direct facial nerve conduction stimulation showed that nine (81.8%) patients had bilateral facial nerve low compound muscle action potential amplitudes. The bilateral blink reflex study showed that eight (88.8%) patients had absent bilateral evoked responses. Finally, the EMG study showed that five (55.5%) patients had active denervation in bilateral sample facial muscles. Conclusions Bilateral facial nerve palsy is an extremely rare condition with a varied etiology. Electrodiagnostic studies are useful in detecting the underlying pathophysiologic processes, prognosis, and central or peripheral lesion localization in patients with facial diplegia.
面神经麻痹的病因多种多样,包括带状疱疹病毒、格林-巴利综合征(GBS)、中耳炎、莱姆病、结节病、人类免疫缺陷病毒等。下运动神经元型面神经麻痹通常由同侧面神经病变引起;然而,也可能由脑桥面神经核和神经束的中枢病变引起。双侧性面瘫是一种极其罕见的病症,在所有面瘫病例中发生率约为0.3%至2.0%。包括直接面神经传导、面部肌电图(EMG)和瞬目反射研究在内的电诊断研究,对面神经麻痹的预后和病变定位很有用。
这项回顾性观察研究在卡塔尔多哈哈马德总医院神经生理学科进行。本研究纳入了11例双侧面部无力并到神经生理学实验室进行电诊断检查的患者。
总共有8例(72.7%)患者出现双侧性面瘫,8例(72.7%)出现反射减退/消失,7例(63.6%)有面部麻木,5例(45.5%)有脑脊液蛋白细胞分离。本研究中双侧性面瘫最常见的病因是GBS(81.9%)。直接面神经传导刺激显示,9例(81.8%)患者双侧面神经复合肌肉动作电位波幅降低。双侧瞬目反射研究显示,8例(88.8%)患者双侧诱发电位消失。最后,肌电图研究显示,5例(55.5%)患者双侧面部样本肌肉有失神经活动。
双侧性面神经麻痹是一种极其罕见的病症,病因多样。电诊断研究有助于检测双侧性面瘫患者潜在的病理生理过程、预后以及中枢或周围病变的定位。