Abdelrahim Maen, Esmail Abdullah, Xu Jiaqiong, Umoru Godsfavour, Al-Rawi Hadeel, Saharia Ashish, Abudayyeh Ala, Victor David, McMillan Robert, Kodali Sudha, Ghobrial Rafik M
Section of GI Oncology Department of Medical Oncology Houston Methodist Cancer Center, Houston, TX, United States.
Cockrell Center of Advanced Therapeutics Phase I program, Houston Methodist Research Institute, Houston, TX, United States.
Front Oncol. 2022 Jun 2;12:908687. doi: 10.3389/fonc.2022.908687. eCollection 2022.
Cholangiocarcinoma management is constantly being updated in view of existing evidence in order to establish practice guidelines and consensus statements. However, the available treatment guidelines to optimize outcomes for cholangiocarcinoma patients who require liver transplantation are still controversial. This study contributing to the cholangiocarcinoma care field by investigating a new promising neoadjuvant therapy that might be help to grant the liver transplant option to the patients with cholangiocarcinoma. Here, we evaluate and compare the potential efficacy of chemotherapy combination of Gemcitabine plus Cisplatin versus non- Gemcitabine and Cisplatin regimens as a neo-adjuvant treatment for cholangiocarcinoma patients prior to liver transplantation.
In this retrospective study, patients with locally advanced, unresectable, hilar, or intrahepatic cholangiocarcinoma with no evidence of extrahepatic disease or vascular involvement were treated with either the combination of neo-adjuvant Gemcitabine plus Cisplatin with no radiation or other standard options of neo-adjuvant treatment. All patients included received chemotherapy prior to being listed for liver transplantation at a single cancer center in collaboration with the same institution's transplant center according to an open-labeled, and centers-approved clinical management protocol. Patients were listed for liver transplantation if they had a minimum of six months of scans showing response or confirmation of disease stability. The primary endpoints were the overall survival and recurrence-free survival after liver transplantation. This report, which was censored on March 18, 2022.
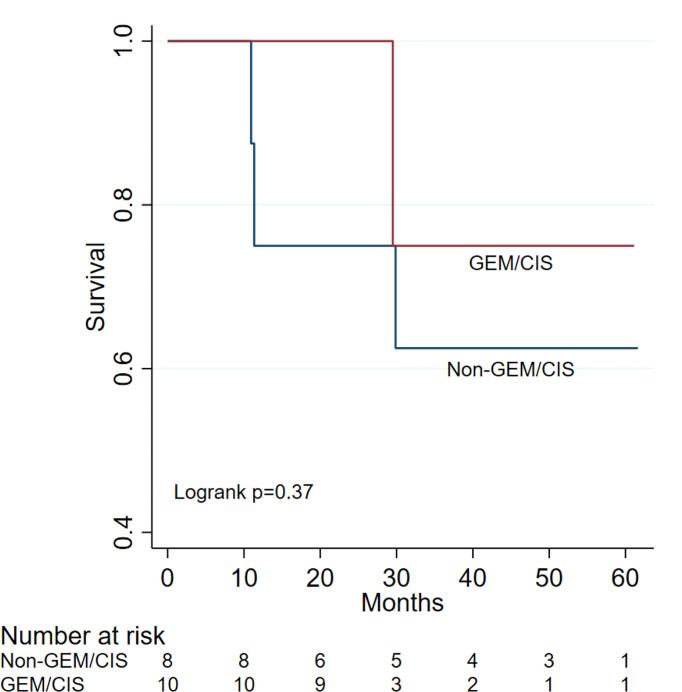
Out of a total of 707 liver transplant recipients were screened, 37 patients were confirmed with a diagnosis of cholangiocarcinoma and only 18 patients (11 males and 7 females) with a median age of 61.83 [interquartile range: 58.27-68.74] met inclusion criteria. Of the 18 patients enrolled, 10 received Gemcitabine/Cisplatin, while 8 patients received either Gemcitabine monotherapy or Capecitabine or FOLFIRI. Months for recurrence after transplantation was 20.1 (IRQ: 20.1-20.1) in the Gemcitabine/Cisplatin group and 9.5 (8.9-12.47) months in the non-Gemcitabine/Cisplatin group (p-value=0.18). Median months of follow-up in the Gemcitabine/Cisplatin group was 28.35 (27.1-32.23) months versus 40.12 (20.6-56.22) months in the non-Gemcitabine/Cisplatin group (p-value=0.33). In non-Gemcitabine/Cisplatin patients, overall survival was 75% (95% CI 31-93%) at both years 1 and 2; 63% (95% CI 23-86%) at years 3 to 5. In Gemcitabine/Cisplatin patients, overall survival was 100% (95% CI 100-100%) at both years 1 and 2; 75% (95% CI 13-96%) at years 3 to 5. Three non-Gemcitabine/Cisplatin patients died at 328 days, 340 days, and 896 days, respectively. One Gemcitabine/Cisplatin patient died at 885 days.
Our findings suggest improved overall survival outcomes with Gemcitabine plus Cisplatin as neo-adjuvant treatment with no concomitant radiation compared to non-Gemcitabine/Cisplatin regimens in patients with cholangiocarcinoma prior to liver transplantation.
鉴于现有证据,胆管癌的治疗方法在不断更新,以制定实践指南和共识声明。然而,对于需要肝移植的胆管癌患者,现有的优化治疗结果的指南仍存在争议。本研究通过调查一种新的有前景的新辅助治疗方法,为胆管癌治疗领域做出贡献,该方法可能有助于为胆管癌患者提供肝移植选择。在此,我们评估并比较吉西他滨联合顺铂化疗方案与非吉西他滨和顺铂方案作为肝移植前胆管癌患者新辅助治疗的潜在疗效。
在这项回顾性研究中,局部晚期、不可切除、肝门部或肝内胆管癌且无肝外疾病或血管受累证据的患者,接受新辅助吉西他滨联合顺铂且不进行放疗的治疗,或接受其他新辅助治疗的标准方案。所有纳入患者在一家癌症中心与同一机构的移植中心合作,根据开放标签且经中心批准的临床管理方案,在列入肝移植名单前接受化疗。如果患者至少有六个月的扫描显示疾病有反应或病情稳定,则将其列入肝移植名单。主要终点是肝移植后的总生存期和无复发生存期。本报告于2022年3月18日进行审查。
在总共筛查的707例肝移植受者中,37例被确诊为胆管癌,只有18例患者(11例男性和7例女性)符合纳入标准,中位年龄为61.83岁[四分位间距:58.27 - 68.74]。在纳入的18例患者中,10例接受吉西他滨/顺铂治疗,而8例患者接受吉西他滨单药治疗或卡培他滨或FOLFIRI治疗。吉西他滨/顺铂组移植后复发时间为20.1个月(四分位间距:20.1 - 20.1),非吉西他滨/顺铂组为9.5个月(8.9 - 12.47)(p值 = 0.18)。吉西他滨/顺铂组的中位随访时间为28.35个月(27.1 - 32.23),非吉西他滨/顺铂组为40.12个月(20.6 - 56.22)(p值 = 0.33)。在非吉西他滨/顺铂组患者中,第1年和第2年的总生存率均为75%(95%置信区间31 - 93%);第3至5年为63%(95%置信区间23 - 86%)。在吉西他滨/顺铂组患者中,第1年和第2年的总生存率均为100%(95%置信区间100 - 100%);第3至5年为75%(95%置信区间13 - 96%)。3例非吉西他滨/顺铂组患者分别在328天、340天和896天死亡。1例吉西他滨/顺铂组患者在885天死亡。
我们的研究结果表明,与非吉西他滨/顺铂方案相比,吉西他滨联合顺铂作为新辅助治疗且不联合放疗,可改善肝移植前胆管癌患者的总生存结局。