Vong Stephen, Chang Jennifer, Assadsangabi Reza, Ivanovic Vladimir
Department of Radiology, UC Davis Health, Sacramento, CA, USA.
Department of Radiology, University of Southern California, Los Angeles, CA, USA.
Neuroradiol J. 2023 Oct;36(5):515-523. doi: 10.1177/19714009221108679. Epub 2022 Jun 18.
Medical errors result in significant mortality and morbidity. The purpose of this study is to analyze skull-base errors at a single tertiary institution, identify common anatomic sites of errors, and offer strategies to reduce errors in this region.
A Neuroradiology Quality Assurance Database of radiologic errors was searched for attending physician computer tomography and magnetic resonance imaging errors in skull-base pathology from 2014 to 2020. Data were limited to CT and MRI reports. Errors were separated into four subcategories (tumor, trauma, vascular, and congenital) and further divided by relevant anatomic site.
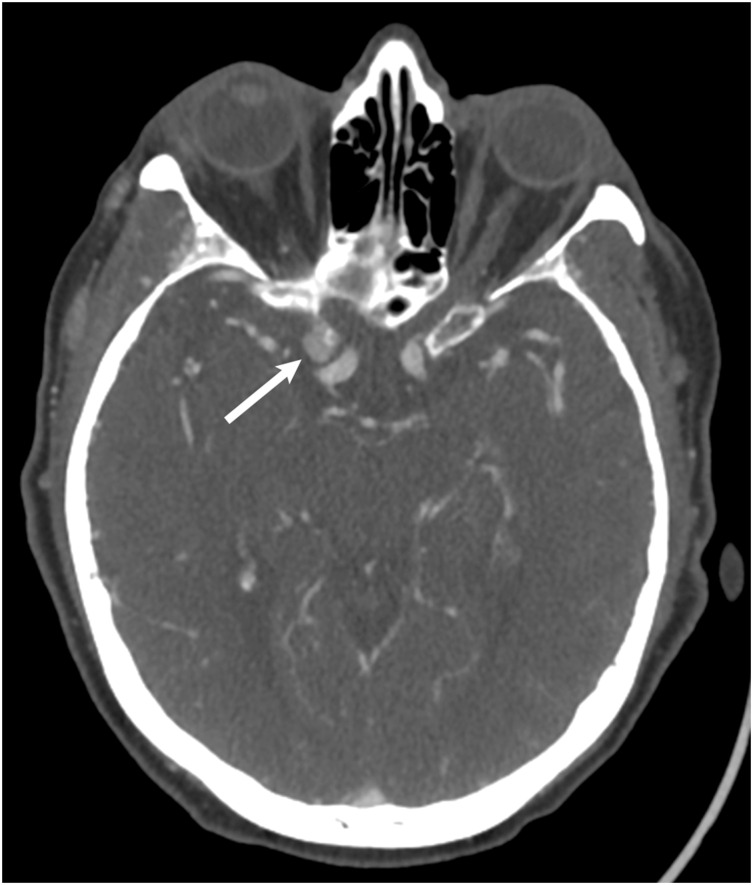
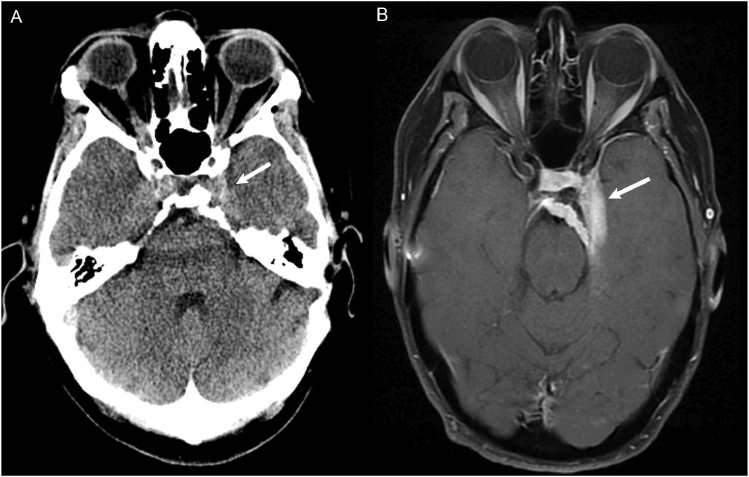
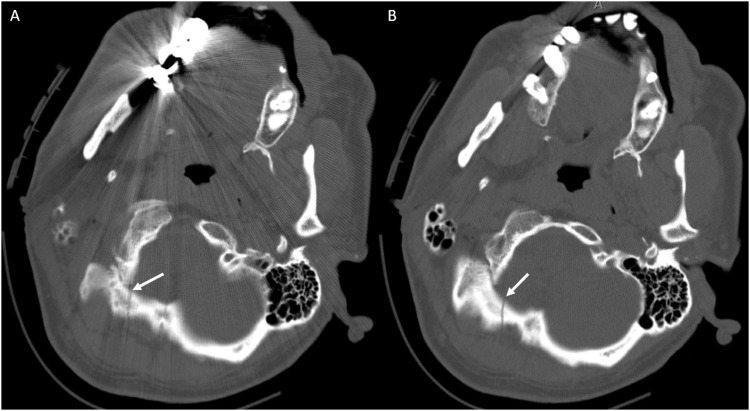
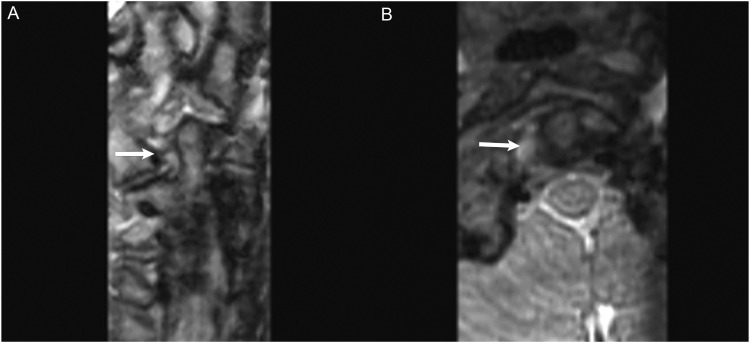
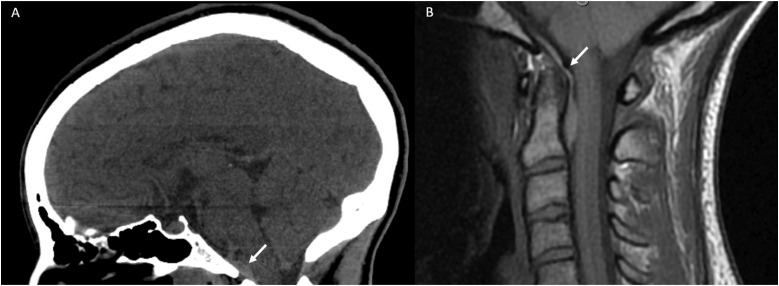
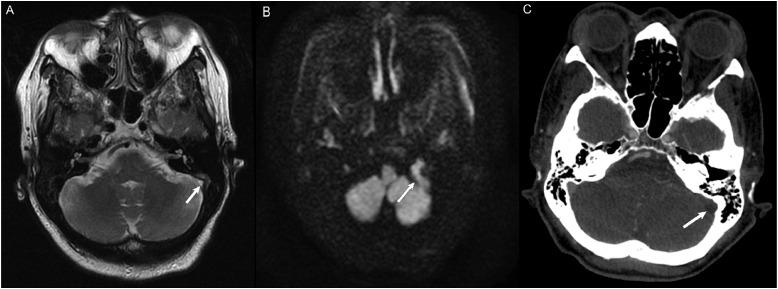
A total of 90 skull-based errors were identified. Most errors were perceptual (87%), with common study types including MRI Brain (39%) and CT Head (24%). Most common errors were tumors (55%), followed by trauma (24%), vascular (10%), and congenital (7%). Six anatomic sites were identified and encompassed over half of errors (58%): sella, occipital bone, cerebellopontine angle/internal auditory canal (CPA/IAC), foramen magnum and clivus, cavernous sinus, and dural venous sinus.
Most of the skull-base errors were perceptual. Placing a strong emphasis on both the pathology and closely examining its critical anatomic site (sella, occipital bone, CPA/IAC, foramen magnum and clivus, cavernous sinus, and dural venous sinus) could potentially reduce up to 60% of errors in these regions.
医疗差错会导致严重的死亡率和发病率。本研究的目的是分析一家三级医疗机构中的颅底差错,确定常见的解剖学差错部位,并提供减少该区域差错的策略。
在一个神经放射学质量保证数据库中搜索2014年至2020年主治医生在颅底病变的计算机断层扫描和磁共振成像中的差错。数据仅限于CT和MRI报告。差错分为四个子类别(肿瘤、创伤、血管和先天性),并进一步按相关解剖部位划分。
共识别出90例颅底差错。大多数差错是感知性的(87%),常见的检查类型包括脑部MRI(39%)和头部CT(24%)。最常见的差错是肿瘤(55%),其次是创伤(24%)、血管(10%)和先天性(7%)。确定了六个解剖部位,这些部位涵盖了一半以上的差错(58%):蝶鞍、枕骨、桥小脑角/内耳道(CPA/IAC)、枕大孔和斜坡、海绵窦和硬脑膜静脉窦。
大多数颅底差错是感知性的。高度重视病变并仔细检查其关键解剖部位(蝶鞍、枕骨、CPA/IAC、枕大孔和斜坡、海绵窦和硬脑膜静脉窦)可能会减少这些区域高达60%的差错。