Center for Healthcare Operations Improvement and Research (CHOIR), University of Twente, Enschede, Overijssel, The Netherlands.
Center for Healthcare Operations Improvement and Research (CHOIR), University of Twente, Enschede, Overijssel, The Netherlands
BMJ Open Qual. 2022 Jun;11(2). doi: 10.1136/bmjoq-2021-001703.
Distancing measures enforced by the COVID-19 pandemic impose a restriction on the number of patients simultaneously present in hospital waiting areas.
Evaluate waiting area occupancy of an intervention that designs clinic blueprint schedules, in which all appointments of the pre-COVID-19 case mix are scheduled either digitally or in person under COVID-19 distancing measures, whereby the number of in-person appointments is maximised.
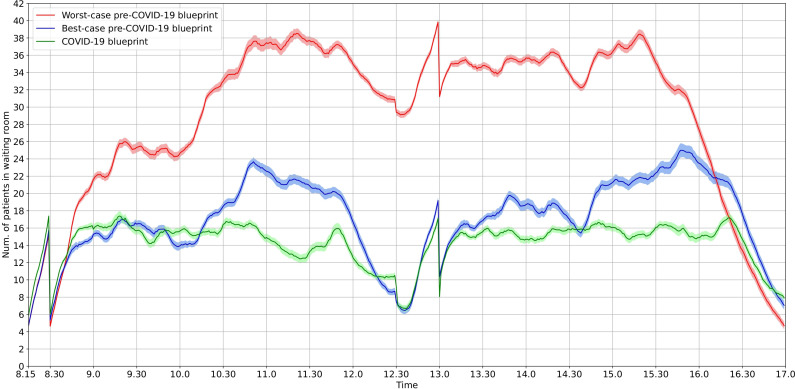
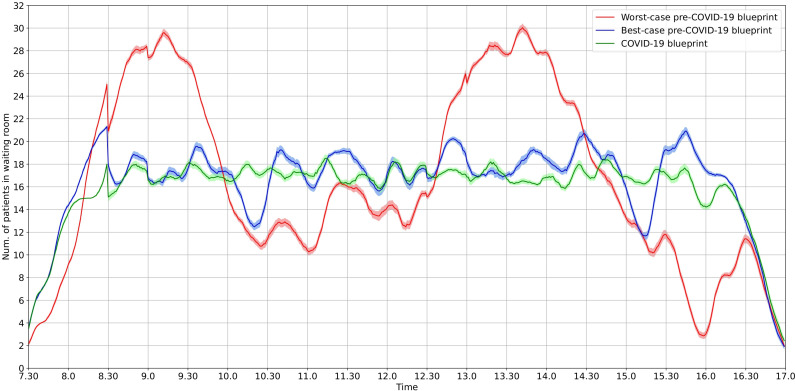
Preintervention analysis and prospective assessment of intervention outcomes were used to evaluate the outcomes on waiting area occupancy and number of in-person consultations (postintervention only) using descriptive statistics, for two settings in the Rheumatology Clinic of Sint Maartenskliniek (SMK) and Medical Oncology & Haematology Outpatient Clinic of University Medical Center Utrecht (UMCU). Retrospective data from October 2019 to February 2020 were used to evaluate the pre-COVID-19 blueprint schedules. An iterative optimisation and simulation approach was followed, based on integer linear programming and Monte Carlo simulation, which iteratively optimised and evaluated blueprint schedules until the 95% CI of the number of patients in the waiting area did not exceed available capacity.
Under pre-COVID-19 blueprint schedules, waiting areas would be overcrowded by up to 22 (SMK) and 11 (UMCU) patients, given the COVID-19 distancing measures. The postintervention blueprint scheduled all appointments without overcrowding the waiting areas, of which 88% and 87% were in person and 12% and 13% were digitally (SMK and UMCU, respectively).
The intervention was effective in two case studies with different waiting area characteristics and a varying number of interdependent patient trajectory stages. The intervention is generically applicable to a wide range of healthcare services that schedule a (series of) appointment(s) for their patients. Care providers can use the intervention to evaluate overcrowding of waiting area(s) and design optimal blueprint schedules to continue a maximum number of in-person appointments under pandemic distancing measures.
COVID-19 大流行实施的隔离措施限制了同时在医院等候区的患者数量。
评估一种干预措施对等候区占用情况的影响,该措施设计了诊所蓝图日程安排,其中所有 COVID-19 大流行前病例组合的预约都在 COVID-19 隔离措施下以数字方式或亲自安排,从而最大限度地增加了亲自预约的数量。
使用描述性统计数据,对 Sint Maartenskliniek(SMK)风湿病诊所和乌得勒支大学医学中心(UMCU)医学肿瘤学和血液学门诊诊所的两个设置进行干预前分析和干预后结果的前瞻性评估,用于评估等候区占用情况和亲自咨询数量(仅在干预后)。使用 2019 年 10 月至 2020 年 2 月的回顾性数据评估 COVID-19 大流行前的蓝图日程安排。采用基于整数线性规划和蒙特卡罗模拟的迭代优化和模拟方法,对蓝图日程安排进行迭代优化和评估,直到等候区的患者数量 95%CI 不超过可用容量。
根据 COVID-19 隔离措施,在 COVID-19 大流行前的蓝图日程安排下,等候区将拥挤多达 22 名(SMK)和 11 名(UMCU)患者。干预后,蓝图安排所有预约,而不会使等候区拥挤,其中 88%和 87%为亲自预约,12%和 13%为数字预约(SMK 和 UMCU 分别)。
该干预措施在具有不同等候区特征和不同数量相互依存患者轨迹阶段的两个案例研究中是有效的。该干预措施普遍适用于为其患者安排(一系列)预约的广泛医疗服务。护理提供者可以使用该干预措施评估等候区的拥挤情况,并设计最佳蓝图日程安排,以便在大流行隔离措施下继续进行最多数量的亲自预约。