Department of Pediatrics, Division of Critical Care Medicine, Nationwide Children's Hospital, The Ohio State University, 700 Children's Drive, Columbus, OH, 43502, USA.
Department of Neurology, George Washington University/Children's National Medical Center, Washington, DC, USA.
Malar J. 2022 Jun 21;21(1):196. doi: 10.1186/s12936-022-04163-0.
Cerebral malaria (CM) results in significant paediatric death and neurodisability in sub-Saharan Africa. Several different alterations to typical Transcranial Doppler Ultrasound (TCD) flow velocities and waveforms in CM have been described, but mechanistic contributors to these abnormalities are unknown. If identified, targeted, TCD-guided adjunctive therapy in CM may improve outcomes.
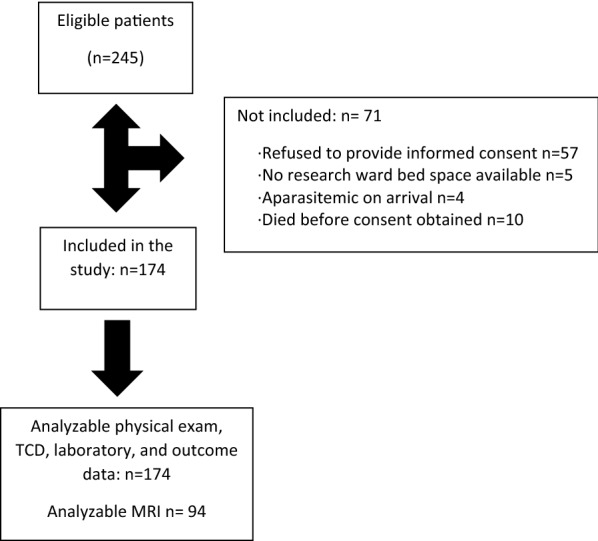
This was a prospective, observational study of children 6 months to 12 years with CM in Blantyre, Malawi recruited between January 2018 and June 2021. Medical history, physical examination, laboratory analysis, electroencephalogram, and magnetic resonance imaging were undertaken on presentation. Admission TCD results determined phenotypic grouping following a priori definitions. Evaluation of the relationship between haemodynamic, metabolic, or intracranial perturbations that lead to these observed phenotypes in other diseases was undertaken. Neurological outcomes at hospital discharge were evaluated using the Paediatric Cerebral Performance Categorization (PCPC) score.
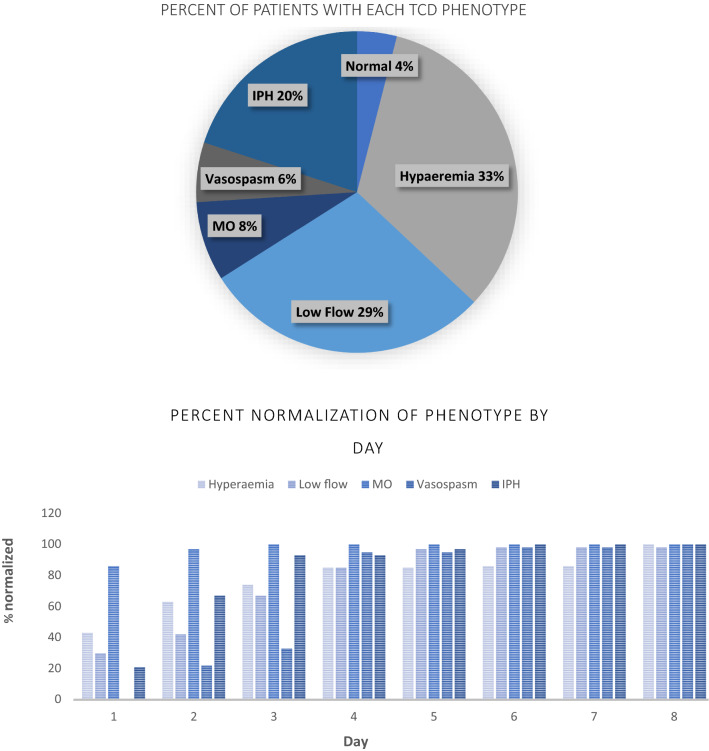
One hundred seventy-four patients were enrolled. Seven (4%) had a normal TCD examination, 57 (33%) met criteria for hyperaemia, 50 (29%) for low flow, 14 (8%) for microvascular obstruction, 11 (6%) for vasospasm, and 35 (20%) for isolated posterior circulation high flow. A lower cardiac index (CI) and higher systemic vascular resistive index (SVRI) were present in those with low flow than other groups (p < 0.003), though these values are normal for age (CI 4.4 [3.7,5] l/min/m2, SVRI 1552 [1197,1961] dscm-5m2). Other parameters were largely not significantly different between phenotypes. Overall, 118 children (68%) had a good neurological outcome. Twenty-three (13%) died, and 33 (19%) had neurological deficits. Outcomes were best for participants with hyperaemia and isolated posterior high flow (PCPC 1-2 in 77 and 89% respectively). Participants with low flow had the least likelihood of a good outcome (PCPC 1-2 in 42%) (p < 0.001). Cerebral autoregulation was significantly better in children with good outcome (transient hyperemic response ratio (THRR) 1.12 [1.04,1.2]) compared to a poor outcome (THRR 1.05 [0.98,1.02], p = 0.05).
Common pathophysiological mechanisms leading to TCD phenotypes in non-malarial illness are not causative in children with CM. Alternative mechanistic contributors, including mechanical factors of the cerebrovasculature and biologically active regulators of vascular tone should be explored.
在撒哈拉以南非洲地区,脑疟疾(CM)可导致儿童死亡和神经残疾。已经描述了 CM 中几种不同的经颅多普勒超声(TCD)血流速度和波形的典型改变,但其异常的机制性贡献尚不清楚。如果能确定这些异常的机制性贡献,并进行有针对性的、TCD 引导的辅助治疗,CM 的预后可能会得到改善。
这是一项在马拉维布兰太尔进行的前瞻性观察性研究,纳入了 2018 年 1 月至 2021 年 6 月期间患有 CM 的 6 个月至 12 岁儿童。在入院时进行了病史、体格检查、实验室分析、脑电图和磁共振成像检查。根据事先定义的标准,TCD 检查结果确定表型分组。研究人员评估了导致其他疾病中这些观察到的表型的血流动力学、代谢或颅内紊乱的关系。出院时使用小儿脑功能分类(PCPC)评分评估神经功能结局。
共纳入了 174 名患者。7 名(4%)患者 TCD 检查正常,57 名(33%)符合充血标准,50 名(29%)符合低血流标准,14 名(8%)符合微血管阻塞标准,11 名(6%)符合血管痉挛标准,35 名(20%)符合孤立性后循环高血流标准。与其他组相比,低血流组的心脏指数(CI)较低,全身血管阻力指数(SVRI)较高(p<0.003),但这些值在年龄上是正常的(CI 4.4[3.7,5]l/min/m2,SVRI 1552[1197,1961]dscm-5m2)。其他参数在表型之间差异不显著。总的来说,118 名儿童(68%)有良好的神经功能结局。23 名(13%)死亡,33 名(19%)有神经功能缺损。充血和孤立性后循环高血流的患者预后最好(分别为 PCPC 1-2 级的比例为 77%和 89%)。低血流组儿童的良好结局比例最低(PCPC 1-2 级的比例为 42%)(p<0.001)。与预后不良的患者相比(THRR 1.05[0.98,1.02]),预后良好的患者的脑自动调节明显更好(THRR 1.12[1.04,1.2])(p=0.05)。
导致非疟疾疾病中 TCD 表型的常见病理生理机制在 CM 儿童中并非是致病因素。应探索其他机制性贡献因素,包括脑血管的机械因素和血管张力的生物活性调节剂。