Department of Applied Tumor Biology, University Hospital Heidelberg Institute of Pathology, Heidelberg, Germany.
Department of Medicine, Weill Cornell Medicine, New York, New York, USA.
J Immunother Cancer. 2022 Jun;10(6). doi: 10.1136/jitc-2021-004416.
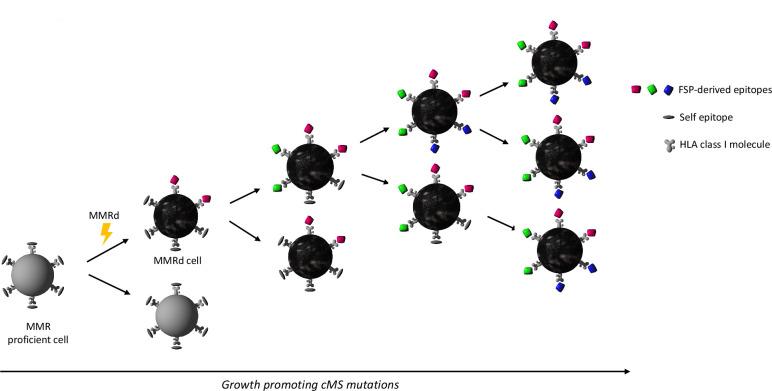
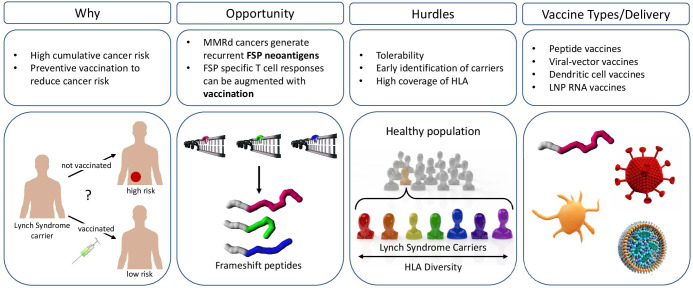
The development of cancer vaccines to induce tumor-antigen specific immune responses was sparked by the identification of antigens specific to or overexpressed in cancer cells. However, weak immunogenicity and the mutational heterogeneity in many cancers have dampened cancer vaccine successes. With increasing information about mutational landscapes of cancers, mutational neoantigens can be predicted computationally to elicit strong immune responses by CD8 +cytotoxic T cells as major mediators of anticancer immune response. Neoantigens are potentially more robust immunogens and have revived interest in cancer vaccines. Cancers with deficiency in DNA mismatch repair have an exceptionally high mutational burden, including predictable neoantigens. Lynch syndrome is the most common inherited cancer syndrome and is caused by DNA mismatch repair gene mutations. Insertion and deletion mutations in coding microsatellites that occur during DNA replication include tumorigenesis drivers. The induced shift of protein reading frame generates neoantigens that are foreign to the immune system. Mismatch repair-deficient cancers and Lynch syndrome represent a paradigm population for the development of a preventive cancer vaccine, as the mutations induced by mismatch repair deficiency are predictable, resulting in a defined set of frameshift peptide neoantigens. Furthermore, Lynch syndrome mutation carriers constitute an identifiable high-risk population. We discuss the pathogenesis of DNA mismatch repair deficient cancers, in both Lynch syndrome and sporadic microsatellite-unstable cancers. We review evidence for pre-existing immune surveillance, the three mechanisms of immune evasion that occur in cancers and assess the implications of a preventive frameshift peptide neoantigen-based vaccine. We consider both preclinical and clinical experience to date. We discuss the feasibility of a cancer preventive vaccine for Lynch syndrome carriers and review current antigen selection and delivery strategies. Finally, we propose RNA vaccines as having robust potential for immunoprevention of Lynch syndrome cancers.
癌症疫苗的发展旨在诱导肿瘤抗原特异性免疫反应,其灵感来自于鉴定在癌细胞中特异性表达或过表达的抗原。然而,许多癌症的免疫原性弱和突变异质性降低了癌症疫苗的成功率。随着关于癌症突变景观的信息不断增加,可以通过计算预测突变新抗原,从而引发 CD8+细胞毒性 T 细胞产生强烈的免疫反应,CD8+细胞毒性 T 细胞是抗癌免疫反应的主要介质。新抗原是潜在的更强大的免疫原,它们重新激发了人们对癌症疫苗的兴趣。缺乏 DNA 错配修复的癌症具有极高的突变负担,包括可预测的新抗原。林奇综合征是最常见的遗传性癌症综合征,由 DNA 错配修复基因突变引起。在 DNA 复制过程中发生的编码微卫星插入和缺失突变包括肿瘤发生驱动因素。蛋白阅读框的诱导移位会产生新抗原,这些新抗原对免疫系统来说是外来的。错配修复缺陷的癌症和林奇综合征代表了开发预防性癌症疫苗的范例人群,因为错配修复缺陷诱导的突变是可预测的,从而产生一组明确的移码肽新抗原。此外,林奇综合征突变携带者构成了可识别的高风险人群。我们讨论了 DNA 错配修复缺陷癌症的发病机制,包括林奇综合征和散发性微卫星不稳定癌症。我们回顾了预先存在的免疫监视的证据,癌症中发生的三种免疫逃避机制,并评估了基于预防性移码肽新抗原的疫苗的影响。我们考虑了迄今为止的临床前和临床经验。我们讨论了林奇综合征携带者癌症预防性疫苗的可行性,并回顾了当前的抗原选择和递送策略。最后,我们提出 RNA 疫苗具有预防林奇综合征癌症的强大潜力。