Divya Gali, Kundal Vijay Kumar, Debnath Pinaki Ranjan, Addagatla Raja Sekhar, Garbhapu Anil Kumar, Saha Arnab Kumar, Meena Atul Kumar, Shah Shalu, Sen Amita
Department of Pediatric Surgery, Atal Bihari Vajpayee Institute of Medical Sciences, Dr. Ram Manohar Lohia Hospital, New Delhi, India.
J Indian Assoc Pediatr Surg. 2022 May-Jun;27(3):293-296. doi: 10.4103/jiaps.JIAPS_19_21. Epub 2022 May 12.
The aim is to study the complications of neonatal thoracotomy and its preventive measures.
We retrospectively reviewed 53 neonates who underwent thoracotomy from January 2017 to December 2019 for a period of 3 years. Patient demographic data, primary disease for which they underwent thoracotomy, postoperative complications (immediate and delayed) during follow-up were documented.
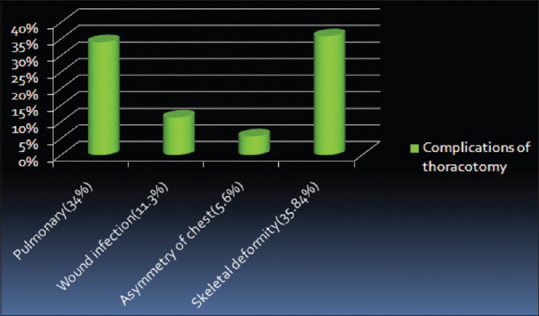
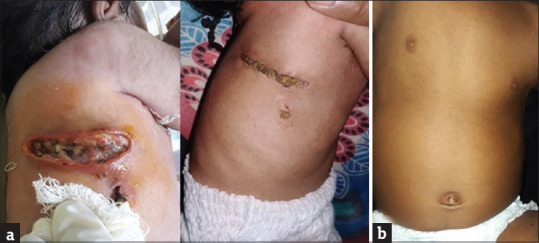
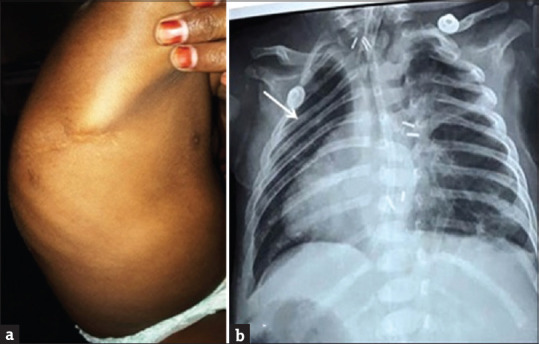
During 3-year period, 53 neonates underwent thoracotomy for various surgical pathologies. The indications were esophageal atresia with tracheoesophageal fistula ( = 49), eventration of diaphragm ( = 3), congenital lobar emphysema of left upper lobe of lung ( = 1). Most of them were right posterolateral thoracotomies ( = 48, 90.56%) and left posterolateral thoracotomy was done in only 5 cases (9.43%). Associated anomalies were seen in 22 cases, such as cardiac ( = 19), renal ( = 4) and gastrointestinal ( = 5). Associated comorbidities seen in 14 cases; preterm ( = 4), low birth weight ( = 13), delayed presentation ( = 6). Early postoperative complications such as pneumonia (34%, n = 18) and wound infection (11.3%, n = 6) were noted. Delayed complications include musculoskeletal abnormalities ( = 19, 35.8%) and esthetic complications such as asymmetry of chest (5.6%).
Neonatal thoracotomy is associated with complications such as pneumonia, wound infections, and musculoskeletal abnormalities such as asymmetry of chest and scoliosis. These can be prevented by adequate postoperative pain relief, muscle-sparing thoracotomies, avoiding tight closures, and nerve injuries. Long-term follow-up is required because these complications may manifest later on also. Early detection and institution of physiotherapy may help.
研究新生儿开胸手术的并发症及其预防措施。
我们回顾性分析了2017年1月至2019年12月期间接受开胸手术的53例新生儿,为期3年。记录了患者的人口统计学数据、接受开胸手术的原发性疾病、随访期间的术后并发症(即刻和延迟)。
在3年期间,53例新生儿因各种手术病理接受了开胸手术。手术指征为食管闭锁合并气管食管瘘(n = 49)、膈膨升(n = 3)、左上叶先天性肺叶气肿(n = 1)。大多数手术采用右后外侧开胸(n = 48,90.56%),仅5例采用左后外侧开胸(9.43%)。22例出现相关畸形,如心脏畸形(n = 19)、肾脏畸形(n = 4)和胃肠道畸形(n = 5)。14例出现相关合并症;早产(n = 4)、低出生体重(n = 13)、就诊延迟(n = 6)。术后早期并发症如肺炎(34%,n = 18)和伤口感染(11.3%,n = 6)。延迟并发症包括肌肉骨骼异常(n = 19,35.8%)和美学并发症如胸廓不对称(5.6%)。
新生儿开胸手术与肺炎、伤口感染以及胸廓不对称和脊柱侧弯等肌肉骨骼异常并发症相关。通过充分的术后疼痛缓解、保留肌肉的开胸手术、避免紧密缝合和神经损伤可预防这些并发症。由于这些并发症可能在后期也会出现,因此需要长期随访。早期发现并进行物理治疗可能会有帮助。