Department of Dermatology, Beijing Tsinghua Changgung Hospital, School of Clinical Medicine, Tsinghua University, Beijing 102218, China.
Department of Plastic, Reconstructive and Aesthetic Surgery, Nippon Medical School, Tokyo 113-8603, Japan.
Int J Mol Sci. 2022 Jun 19;23(12):6820. doi: 10.3390/ijms23126820.
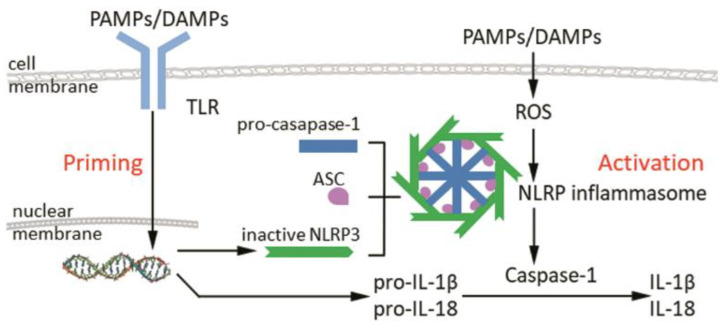
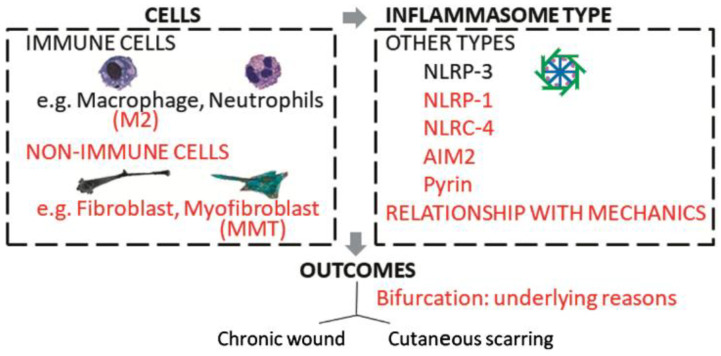
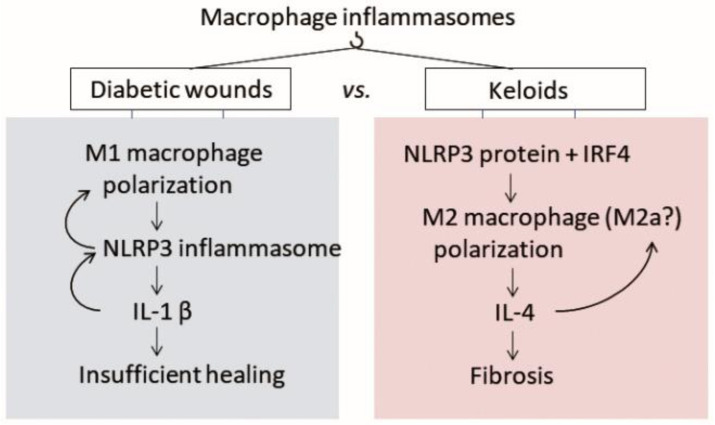
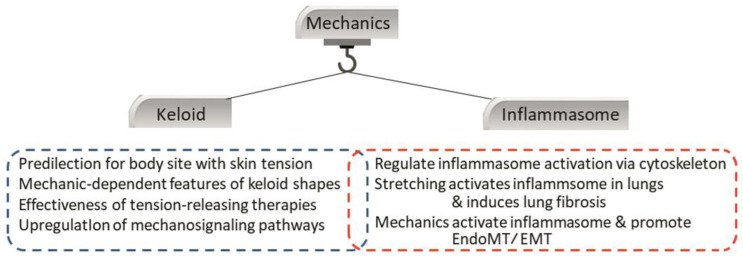
Keloids and hypertrophic scars are pathological cutaneous scars. They arise from excessive wound healing, which induces chronic dermal inflammation and results in overwhelming fibroblast production of extracellular matrix. Their etiology is unclear. Inflammasomes are multiprotein complexes that are important in proinflammatory innate-immune system responses. We asked whether inflammasomes participate in pathological scarring by examining the literature on scarring, diabetic wounds (also characterized by chronic inflammation), and systemic sclerosis (also marked by fibrosis). Pathological scars are predominantly populated by anti-inflammatory M2 macrophages and recent literature hints that this could be driven by non-canonical inflammasome signaling. Diabetic-wound healing associates with inflammasome activation in immune (macrophages) and non-immune (keratinocytes) cells. Fibrotic conditions associate with inflammasome activation and inflammasome-induced transition of epithelial cells/endothelial cells/macrophages into myofibroblasts that deposit excessive extracellular matrix. Studies suggest that mechanical stimuli activate inflammasomes via the cytoskeleton and that mechanotransduction-inflammasome crosstalk is involved in fibrosis. Further research should examine (i) the roles that various inflammasome types in macrophages, (myo)fibroblasts, and other cell types play in keloid development and (ii) how mechanical stimuli interact with inflammasomes and thereby drive scar growth. Such research is likely to significantly advance our understanding of pathological scarring and aid the development of new therapeutic strategies.
瘢痕疙瘩和增生性瘢痕是病理性皮肤瘢痕。它们是由过度的伤口愈合引起的,这会导致慢性真皮炎症,并导致成纤维细胞产生大量细胞外基质。它们的病因尚不清楚。炎症小体是多蛋白复合物,在促炎固有免疫系统反应中起重要作用。我们通过检查有关瘢痕形成、糖尿病伤口(也以慢性炎症为特征)和系统性硬化症(也以纤维化为特征)的文献,来研究炎症小体是否参与病理性瘢痕形成。病理性瘢痕主要由抗炎性 M2 巨噬细胞组成,最近的文献表明,这可能是由非经典炎症小体信号驱动的。糖尿病伤口愈合与免疫(巨噬细胞)和非免疫(角质形成细胞)细胞中的炎症小体激活有关。纤维化状态与炎症小体激活以及上皮细胞/内皮细胞/巨噬细胞向产生过多细胞外基质的肌成纤维细胞的炎症小体诱导转化有关。研究表明,机械刺激通过细胞骨架激活炎症小体,并且机械转导-炎症小体串扰参与纤维化。进一步的研究应该检查(i)各种炎症小体类型在巨噬细胞、(肌成纤维细胞)和其他细胞类型中在瘢痕疙瘩发展中的作用,以及 (ii)机械刺激如何与炎症小体相互作用,从而驱动瘢痕生长。这种研究很可能会极大地提高我们对病理性瘢痕形成的理解,并有助于开发新的治疗策略。