Lin Jia-Ling, Tseng Wei-Kung, Lee Po-Tseng, Lee Cheng-Han, Tseng Shih-Ya, Chen Po-Wei, Chang Hsien-Yuan, Chao Ting-Hsing
Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan 704302, Taiwan.
Department of Internal Medicine, National Cheng Kung University Hospital, Dou-Liou Branch, College of Medicine, National Cheng Kung University, Yunlin 640003, Taiwan.
J Pers Med. 2022 Jun 6;12(6):938. doi: 10.3390/jpm12060938.
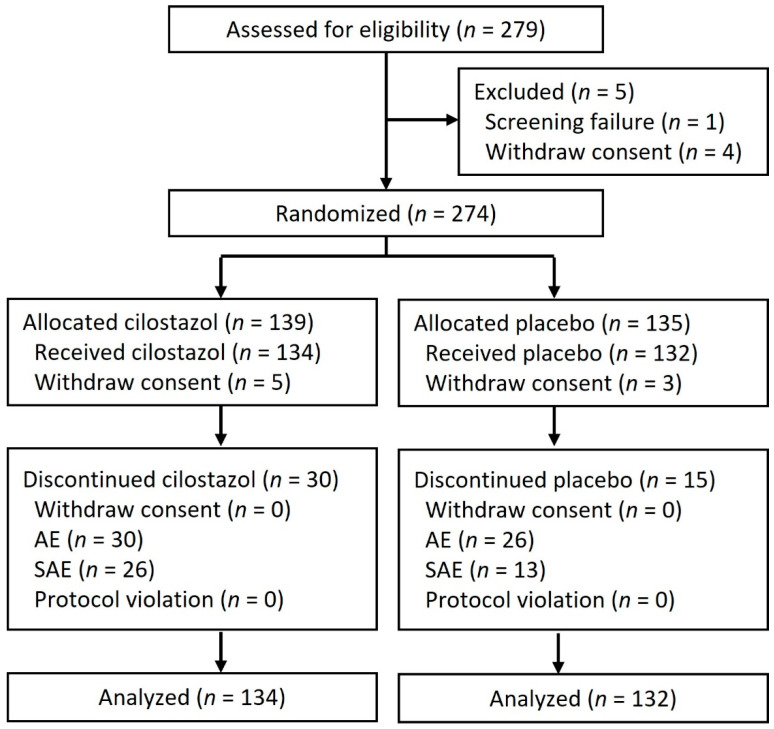
Previous studies found that cilostazol has a favorable effect on glucose and lipid homeostasis, endothelial function, atherosclerosis, and vasculo-angiogenesis. However, it is poorly understood whether these effects can translate into better clinical outcomes. This study investigated the outcome effect of cilostazol in patients with coronary artery disease (CAD) or at a high risk of cardiovascular (CV) disease. We conducted a randomized, double-blind, placebo-controlled trial involving 266 patients who received cilostazol, 200 mg/day ( = 134) or placebo ( = 132). Pre-specified clinical endpoints including composite major adverse cardiovascular events (MACE) (CV death, non-fatal myocardial infarct, non-fatal stroke, hospitalization for heart failure, or unplanned coronary revascularization), the composite major coronary event (MCE) and major adverse CV and cerebrovascular event (MACCE), were prospectively assessed. The mean duration of follow-up was 2.9 years. Relative to placebo, cilostazol treatment had a borderline effect on risk reduction of MACE (hazard ratio [HR], 0.67; 95% confidence interval (CI), 0.34-1.33), whereas the beneficial effect in favor of cilostazol was significant in patients with diabetes mellitus or a history of percutaneous coronary intervention ( for interaction, 0.02 and 0.06, respectively). Use of cilostazol, significantly reduced the risk of MCE (HR, 0.38; 95% CI, 0.17-0.86) and MACCE (HR, 0.47; 95% CI, 0.23-0.96). A significantly lower risk of angina pectoris (HR, 0.38; 95% CI, 0.17-0.86) was also observed in the cilostazol group. After multi-variable adjustment, cilostazol treatment independently predicted a lower risk of MCE. In conclusion, these results suggest cilostazol may have beneficial effects in patients with CAD or at a high risk of CV disease.
既往研究发现,西洛他唑对血糖和脂质稳态、内皮功能、动脉粥样硬化及血管生成具有有益作用。然而,这些作用能否转化为更好的临床结局,目前尚不清楚。本研究调查了西洛他唑对冠心病(CAD)患者或心血管(CV)疾病高危患者的结局影响。我们进行了一项随机、双盲、安慰剂对照试验,纳入266例患者,其中134例接受西洛他唑200mg/天治疗,132例接受安慰剂治疗。预先设定的临床终点包括复合主要不良心血管事件(MACE)(CV死亡、非致死性心肌梗死、非致死性卒中、因心力衰竭住院或计划外冠状动脉血运重建)、复合主要冠状动脉事件(MCE)以及主要不良CV和脑血管事件(MACCE),并进行前瞻性评估。平均随访时间为2.9年。与安慰剂相比,西洛他唑治疗对降低MACE风险有临界效应(风险比[HR],0.67;95%置信区间[CI],0.34 - 1.33),而在糖尿病患者或有经皮冠状动脉介入治疗史的患者中,西洛他唑的有益作用显著(交互作用P值分别为0.02和0.06)。使用西洛他唑可显著降低MCE风险(HR,0.38;95% CI,0.17 - 0.86)和MACCE风险(HR,0.47;95% CI,0.23 - 0.96)。在西洛他唑组中还观察到心绞痛风险显著降低(HR,0.38;95% CI,0.17 - 0.86)。经过多变量调整后,西洛他唑治疗独立预测MCE风险较低。总之,这些结果表明西洛他唑可能对CAD患者或CV疾病高危患者具有有益作用。