Prins Hendrik J, Duijkers Ruud, Kramer Gerdien, Boerhout Els, Rietema Floris J, de Jong Pim A, Schoorl Marianne I, van der Werf Tjip S, Boersma Wim G
Dept Pulmonary Diseases, Northwest Hospital, Alkmaar, the Netherlands.
Dept Radiology, Northwest Hospital, Alkmaar, the Netherlands.
ERJ Open Res. 2022 Jun 20;8(2). doi: 10.1183/23120541.00054-2022. eCollection 2022 Apr.
Acute exacerbations of COPD (AECOPD) and community acquired pneumonia (CAP) often coexist. Although chest radiographs may differentiate between these diagnoses, chest radiography is known to underestimate the incidence of CAP in AECOPD. In this exploratory study, we prospectively investigated the incidence of infiltrative changes using low-dose computed tomography (LDCT). Additionally, we investigated whether clinical biomarkers of CAP differed between patients with and without infiltrative changes.
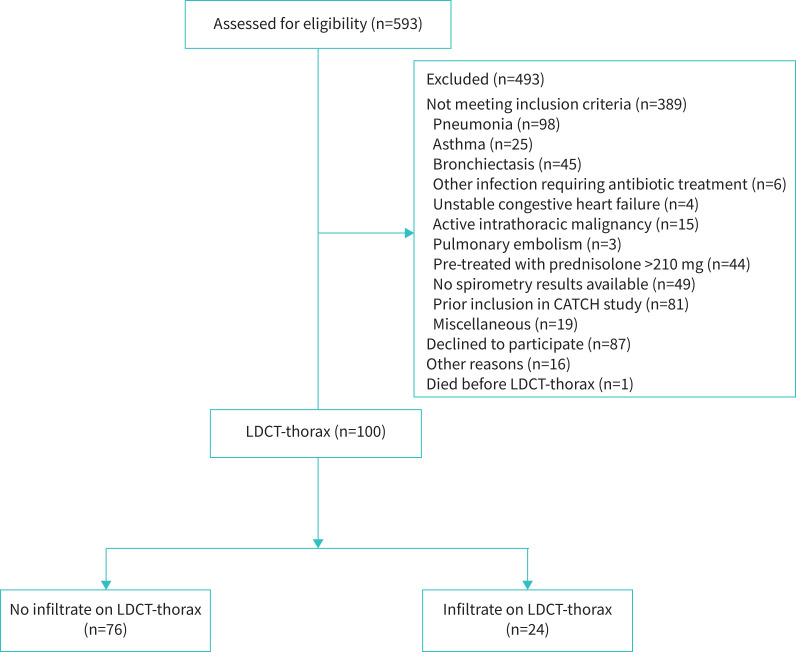
Patients with AECOPD in which pneumonia was excluded using chest radiography underwent additional LDCT-thorax. The images were read independently by two radiologists; a third radiologist was consulted as adjudicator. C-reactive protein (CRP), procalcitonin (PCT), and serum amyloid A (SAA) at admission were assessed.
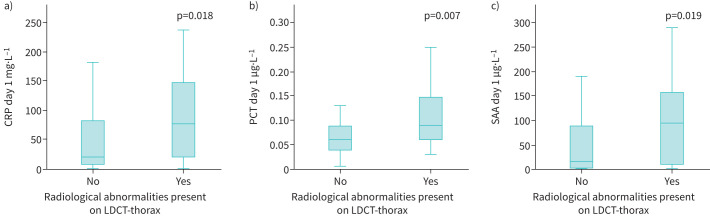
Out of the 100 patients included, 24 had one or more radiographic abnormalities suggestive of pneumonia. The interobserver agreement between two readers (Cohen's κ) was 0.562 (95% CI 0.371-0.752; p<0.001). Biomarkers were elevated in the group with radiological abnormalities compared to the group without abnormalities. Median (interquartile range (IQR)) CRP was 76 (21.5-148.0) mg·L compared to 20.5 (8.8-81.5) mg·L (p=0.018); median (IQR) PCT was 0.09 (0.06-0.15) µg·L compared to 0.06 (0.04-0.08) μg·L (p=0.007); median (IQR) SAA was 95 (7-160) µg·mL compared to 16 (3-89) µg·mL (p=0.019). Sensitivity and specificity for all three biomarkers were moderate for detecting radiographic abnormalities by LDCT in this population. The area under the receiver operating characteristic curve was 0.66 (95% CI 0.52-0.80) for CRP, 0.66 (95% CI 0.53-0.80) for PCT and 0.69 (95% CI 0.57-0.81) for SAA.
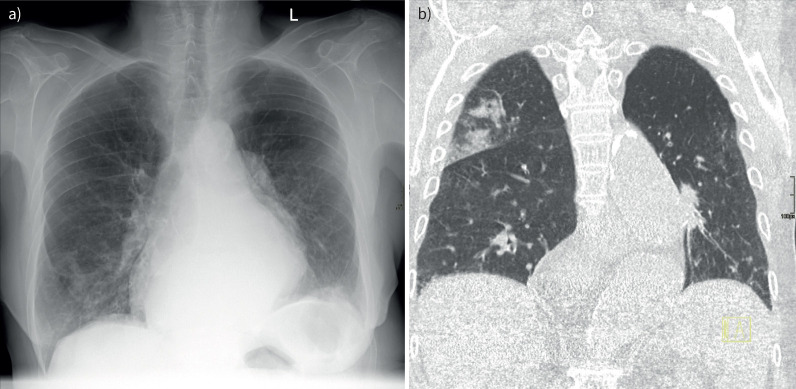
LDCT can detect additional radiological abnormalities that may indicate acute-phase lung involvement in patients with AECOPD without infiltrate(s) on the chest radiograph. Despite CRP, PCT and SAA being significantly higher in the group with radiological abnormalities on LDCT, they proved unable to reliably detect or exclude CAP. Further research is warranted.
慢性阻塞性肺疾病急性加重(AECOPD)与社区获得性肺炎(CAP)常并存。虽然胸部X线片可区分这些诊断,但已知胸部X线摄影会低估AECOPD中CAP的发病率。在这项探索性研究中,我们前瞻性地研究了使用低剂量计算机断层扫描(LDCT)检测浸润性改变的发生率。此外,我们还研究了有和没有浸润性改变的患者之间CAP的临床生物标志物是否存在差异。
通过胸部X线片排除肺炎的AECOPD患者接受了额外的胸部LDCT检查。图像由两名放射科医生独立阅片;第三名放射科医生作为裁决者进行会诊。评估入院时的C反应蛋白(CRP)、降钙素原(PCT)和血清淀粉样蛋白A(SAA)。
在纳入的100例患者中,24例有一项或多项提示肺炎的影像学异常。两位阅片者之间的观察者间一致性(Cohen's κ)为0.562(95%CI 0.371 - 0.752;p<0.001)。与无异常组相比,有放射学异常组的生物标志物升高。CRP的中位数(四分位间距(IQR))为76(21.5 - 148.0)mg·L,而无异常组为20.5(8.8 - 81.5)mg·L(p = 0.018);PCT中位数(IQR)为0.09(0.06 - 0.15)μg·L,无异常组为0.06(0.04 - 0.08)μg·L(p = 0.007);SAA中位数(IQR)为95(7 - 160)μg·mL,无异常组为16(3 - 89)μg·mL(p = 0.019)。在该人群中,所有三种生物标志物检测LDCT影像学异常的敏感性和特异性均为中等。CRP的受试者工作特征曲线下面积为0.66(95%CI 0.52 - 0.80),PCT为0.66(95%CI 0.53 - 0.80),SAA为0.69(95%CI 0.57 - 0.81)。
LDCT可以检测到额外的放射学异常,这些异常可能表明胸部X线片无浸润的AECOPD患者存在急性期肺部受累。尽管LDCT上有放射学异常组的CRP、PCT和SAA显著更高,但它们无法可靠地检测或排除CAP。有必要进行进一步研究。