Institute of Cardiology, ASST Spedali Civili, Department of Medical and Surgical Specialties, Radiological Sciences and Public Health, University of Brescia, Brescia, Italy.
Division of Cardiology and Metabolism, Department of Cardiology (CVK) and Berlin-Brandenburg Center for Regenerative Therapies (BCRT), German Centre for Cardiovascular Research (DZHK) Partner Site Berlin, Charité Universitätsmedizin Berlin, Berlin, Germany.
Eur J Heart Fail. 2022 Nov;24(11):2131-2139. doi: 10.1002/ejhf.2593. Epub 2022 Jul 12.
Limited data exist regarding the prognostic relevance of changes in left atrial (LA) dimensions in patients with heart failure (HF). We assessed changes in LA dimension and their relation with outcomes after optimization of guideline-directed medical therapy (GDMT) in patients with new-onset or worsening HF.
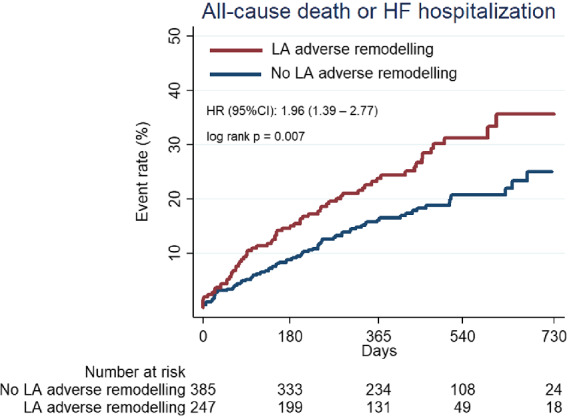
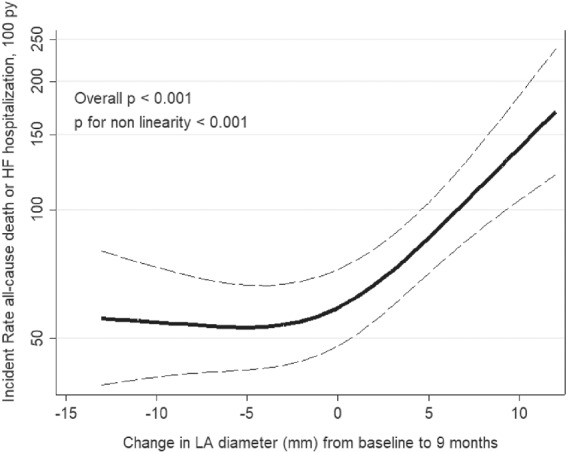
Left atrial diameter was assessed at baseline and 9 months after GDMT optimization in 632 patients (mean age 65.8 ± 12.1 years, 22.3% female) enrolled in BIOSTAT-CHF. LA adverse remodelling (LAAR) was defined as an increase in LA diameter on transthoracic echocardiography between baseline and 9 months. After the 9-month visit, patients were followed for a median of 13 further months. LAAR was observed in 247 patients (39%). Larger baseline LA diameter (odds ratio [OR] 0.90; 95% confidence interval [CI] 0.87-0.93; p < 0.001) and up-titration to higher doses of angiotensin-converting enzyme inhibitors or angiotensin receptor blockers (ACEi/ARBs) (OR 0.56; 95% CI 0.34-0.92; p = 0.022) were independently associated with lower likelihood of LAAR. LAAR was associated with an increased risk of the composite of all-cause mortality or HF hospitalization (log-rank p = 0.007 and adjusted hazard ratio 1.73, 95% CI 1.22-2.45, p = 0.002). The association was more pronounced in patients without a history of atrial fibrillation (p for interaction = 0.009).
Among patients enrolled in BIOSTAT-CHF, LAAR was associated with an unfavourable outcome and was prevented by ACEi/ARB up-titration. Changes in LA dimension may be a useful marker of response to treatment and improve risk stratification in patients with HF.
心力衰竭(HF)患者左心房(LA)大小变化的预后相关性数据有限。我们评估了新出现或恶化的 HF 患者接受指南指导的药物治疗(GDMT)优化后 LA 大小的变化及其与结局的关系。
在 BIOSTAT-CHF 中,632 名新发病或恶化 HF 患者(平均年龄 65.8±12.1 岁,22.3%为女性)接受 GDMT 优化前后分别评估了 LA 直径。LA 不良重构(LAAR)定义为经胸超声心动图基线和 9 个月时 LA 直径增加。9 个月就诊后,中位随访 13 个月。247 名患者(39%)出现 LAAR。较大的基线 LA 直径(比值比 [OR] 0.90;95%置信区间 [CI] 0.87-0.93;p<0.001)和 ACEi/ARBs 剂量上调(OR 0.56;95%CI 0.34-0.92;p=0.022)与 LAAR 的可能性降低独立相关。LAAR 与全因死亡率或 HF 住院的复合终点风险增加相关(对数秩检验 p=0.007,调整后的危险比 1.73,95%CI 1.22-2.45,p=0.002)。在没有房颤病史的患者中,这种相关性更为显著(p 交互=0.009)。
在 BIOSTAT-CHF 中入组的患者中,LAAR 与不良结局相关,通过 ACEi/ARB 剂量上调可以预防 LAAR。LA 大小的变化可能是 HF 患者对治疗反应的有用标志物,并改善风险分层。