Chevalier Laurent, Cochet Hubert, Mahida Saagar, S Sylvain Blanchard, Benard Antoine, Cariou Tanguy, Sridi-Cheniti Soumaya, Benhenda Samy, Doutreleau Stéphane, Cade Stéphane, Guerard Sylvain, Guy Jean-Michel, Trimoulet Pascale, Picard Stéphane, Dusfour Bernard, Pouzet Aurelie, Roseng Stéphanie, Franchi Marco, Jaïs Pierre, Pellegrin Isabelle
Clinique du Sport Bordeaux-Mérignac, 2 rue Georges Negrevergne, 33700, Merignac, France.
IHU Liryc, CHU Bordeaux, Univ. Bordeaux, Bordeaux, France.
Sports Med Open. 2022 Jun 25;8(1):83. doi: 10.1186/s40798-022-00469-0.
There is a paucity of data on cardiovascular sequelae of asymptomatic/mildly symptomatic SARS-Cov-2 infections (COVID).
The aim of this prospective study was to characterize the cardiovascular sequelae of asymptomatic/mildly symptomatic COVID-19 among high/elite-level athletes.
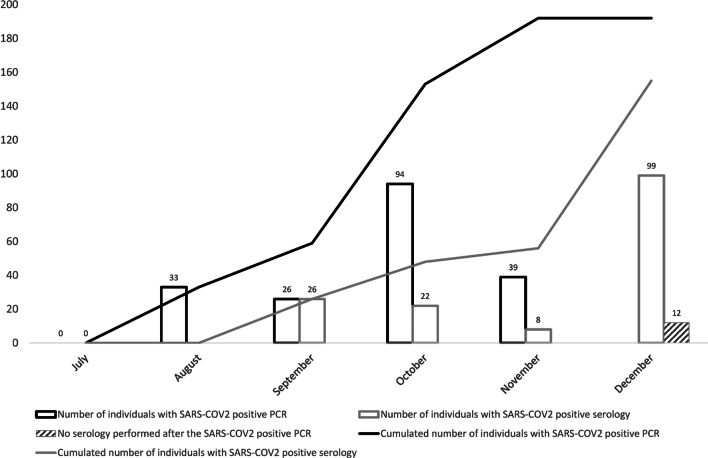
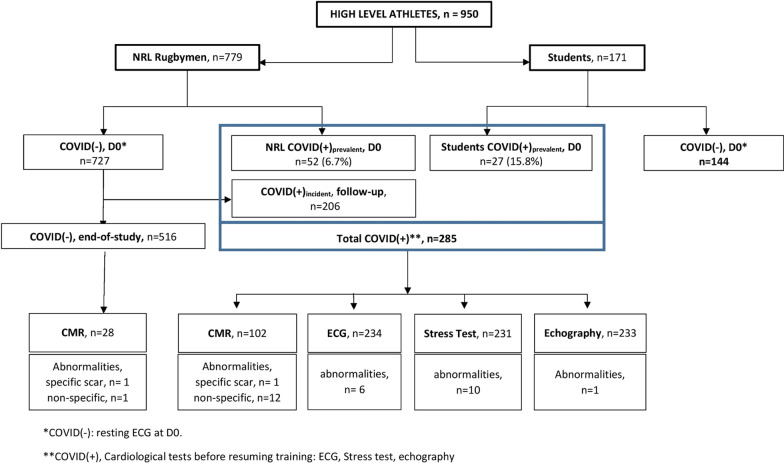
950 athletes (779 professional French National Rugby League (F-NRL) players; 171 student athletes) were included. SARS-Cov-2 testing was performed at inclusion, and F-NRL athletes were intensely followed-up for incident COVID-19. Athletes underwent ECG and biomarker profiling (D-Dimer, troponin, C-reactive protein). COVID(+) athletes underwent additional exercise testing, echocardiography and cardiac magnetic resonance imaging (CMR).
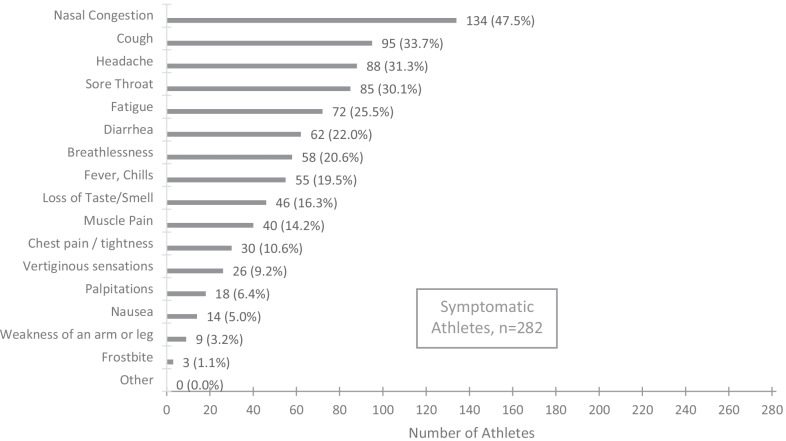
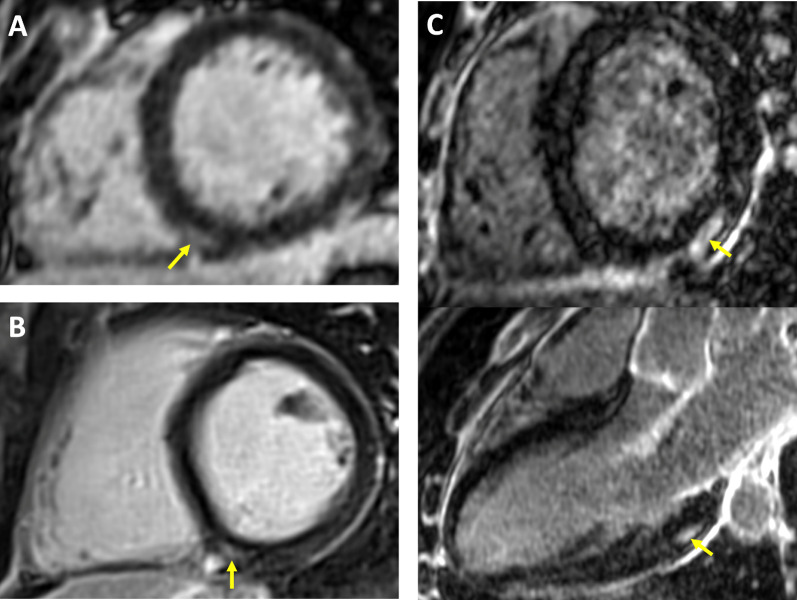
285/950 athletes (30.0%) had mild/asymptomatic COVID-19 [79 (8.3%) at inclusion (COVID(+)); 206 (28.3%) during follow-up (COVID(+))]. 2.6% COVID(+) athletes had abnormal ECGs, while 0.4% had an abnormal echocardiogram. During stress testing (following 7-day rest), COVID(+) athletes had a functional capacity of 12.8 ± 2.7 METS with only stress-induced premature ventricular ectopy in 10 (4.3%). Prevalence of CMR scar was comparable between COVID(+) athletes and controls [COVID(+) vs. COVID(-); 1/102 (1.0%) vs 1/28 (3.6%)]. During 289 ± 56 days follow-up, one athlete had ventricular tachycardia, with no obvious link with a SARS-CoV-2 infection. The proportion with troponin I and CRP values above the upper-limit threshold was comparable between pre- and post-infection (5.9% vs 5.9%, and 5.6% vs 8.7%, respectively). The proportion with D-Dimer values above the upper-limit threshold increased when comparing pre- and post-infection (7.9% vs 17.3%, P = 0.01).
The absence of cardiac sequelae in pauci/asymptomatic COVID(+) athletes is reassuring and argues against the need for systematic cardiac assessment prior to resumption of training (clinicaltrials.gov; NCT04936503).
关于无症状/轻度症状的严重急性呼吸综合征冠状病毒2(SARS-CoV-2)感染(新冠病毒感染)的心血管后遗症的数据较少。
这项前瞻性研究的目的是描述高水平/精英级运动员中无症状/轻度症状新冠病毒感染的心血管后遗症。
纳入950名运动员(779名法国国家职业橄榄球联盟(F-NRL)运动员;171名学生运动员)。在纳入时进行SARS-CoV-2检测,对F-NRL运动员进行密切随访以观察新冠病毒感染情况。运动员接受心电图和生物标志物分析(D-二聚体、肌钙蛋白、C反应蛋白)。新冠病毒检测呈阳性(COVID(+))的运动员接受额外的运动测试、超声心动图和心脏磁共振成像(CMR)。
950名运动员中有285名(30.0%)患有轻度/无症状新冠病毒感染[纳入时79名(8.3%)(COVID(+));随访期间206名(28.3%)(COVID(+))]。2.6%的COVID(+)运动员心电图异常,而0.4%的运动员超声心动图异常。在压力测试期间(休息7天后),COVID(+)运动员的功能能力为12.8±2.7代谢当量,只有10名(4.3%)出现压力诱发的室性早搏。COVID(+)运动员和对照组的CMR疤痕患病率相当[COVID(+)与COVID(-);1/102(1.0%)与1/28(3.6%)]。在289±56天的随访期间,一名运动员出现室性心动过速,与SARS-CoV-2感染无明显关联。感染前和感染后肌钙蛋白I和CRP值高于上限阈值的比例相当(分别为5.9%对5.9%,5.6%对8.7%)。比较感染前和感染后,D-二聚体值高于上限阈值的比例增加(7.9%对17.3%,P=0.01)。
轻度/无症状COVID(+)运动员无心脏后遗症令人安心,这表明在恢复训练前无需进行系统性心脏评估(clinicaltrials.gov;NCT04936503)。