Unit of Internal Medicine and Metabolic Diseases, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, Milan, Italy.
Department of Pathophysiology and Transplantation, Università Degli Studi di Milano, Via F. SFORZA 35, 20122, Milan, Italy.
Intern Emerg Med. 2022 Sep;17(6):1739-1749. doi: 10.1007/s11739-022-03000-1. Epub 2022 Jun 26.
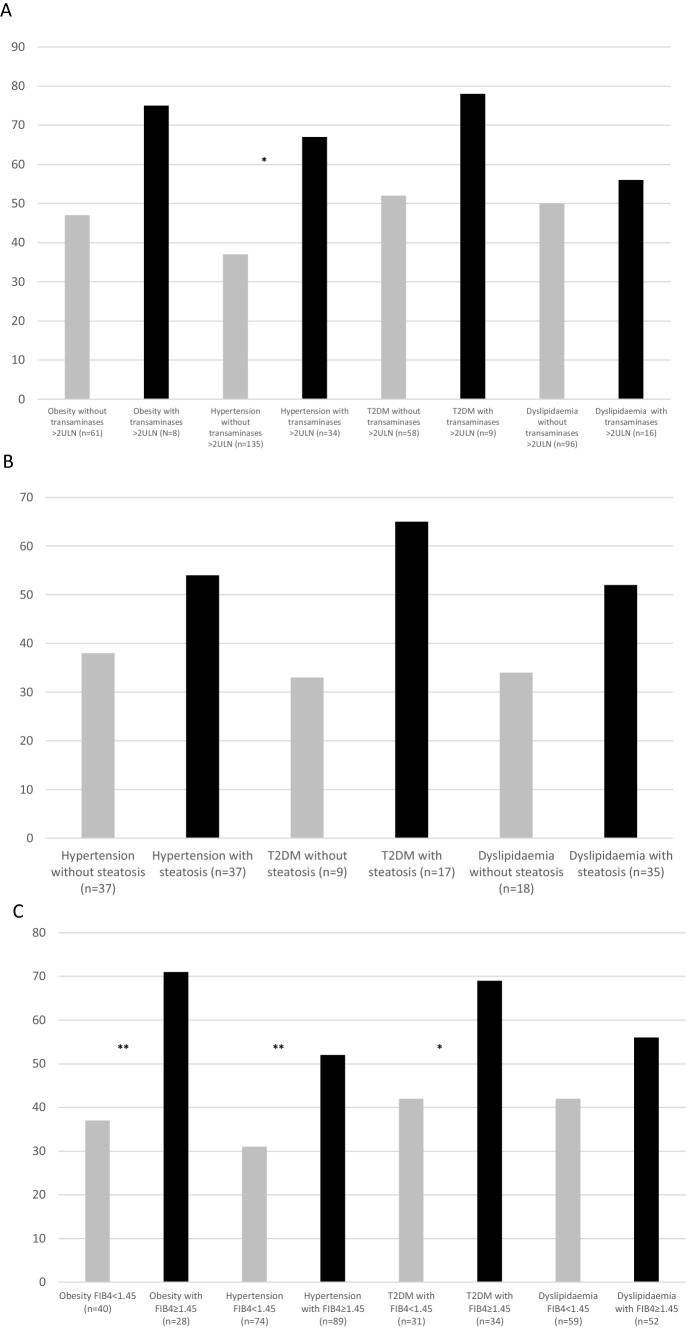
Despite vaccination programs, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection remains a public health problem. Identifying key prognostic determinants of severity of the disease may help better focus health resources. The negative prognostic role for metabolic and hepatic alterations is established; however, the interplay among different metabolic comorbidities and their interconnections with the liver have never been explored.The objective of this study is to evaluate the impact of liver alterations in addition to metabolic comorbidities as a predictor of SARS-CoV-2 severity. 382 SARS-CoV-2 patients were enrolled. Severe SARS-CoV-2 was diagnosed according to international consensus. Transaminases > 2 times the upper limit of normality (2ULN), hepatic steatosis (by ultrasound and/or computed tomography in 133 patients), and FIB-4 defined liver alterations. All data were collected on admission. The results are severe SARS-CoV-2 infection in 156 (41%) patients (mean age 65 ± 17; 60%males). Prevalence of obesity was 25%; diabetes, 17%; hypertension, 44%; dyslipidaemia, 29%; with 13% of the cohort with ≥ 3 metabolic alterations. Seventy patients (18%) had transaminases > 2ULN, 82 (62%) steatosis; 199 (54%) had FIB-4 < 1.45 and 45 (12%) > 3.25. At multivariable analysis, ≥ 3 metabolic comorbidities (OR 4.1, CI 95% 1.8-9.1) and transaminases > 2ULN (OR 2.6, CI 95% 1.3-6.7) were independently associated with severe SARS-CoV-2. FIB-4 < 1.45 was a protective factor (OR 0.42, CI 95% 0.23-0.76). Hepatic steatosis had no impact on disease course. The presence of metabolic alterations is associated with severe SARS-CoV-2 infection, and the higher the number of coexisting comorbidities, the higher the risk of severe disease. Normal FIB-4 values are inversely associated with advanced SARS-CoV-2 regardless of metabolic comorbidities, speculating on use of these values to stratify the risk of severe infection.
尽管有疫苗接种计划,但严重急性呼吸综合征冠状病毒 2 (SARS-CoV-2) 感染仍然是一个公共卫生问题。确定疾病严重程度的关键预后决定因素可能有助于更好地集中卫生资源。代谢和肝脏改变的负面预后作用已得到确立;然而,不同代谢合并症之间的相互作用及其与肝脏的相互联系从未被探索过。本研究的目的是评估除代谢合并症外,肝脏改变作为 SARS-CoV-2 严重程度预测因子的作用。共纳入 382 例 SARS-CoV-2 患者。根据国际共识诊断严重 SARS-CoV-2。转氨酶>正常值上限 2 倍(2ULN)、肝脂肪变性(133 例患者通过超声和/或计算机断层扫描)和 FIB-4 定义的肝脏改变。所有数据均在入院时收集。结果显示 156 例(41%)患者感染严重 SARS-CoV-2(平均年龄 65±17;60%为男性)。肥胖患病率为 25%;糖尿病患病率为 17%;高血压患病率为 44%;血脂异常患病率为 29%;有 13%的患者存在≥3 种代谢异常。70 例(18%)患者转氨酶>2ULN,82 例(62%)患者存在脂肪变性;199 例(54%)患者 FIB-4<1.45,45 例(12%)患者 FIB-4>3.25。多变量分析显示,≥3 种代谢合并症(OR 4.1,95%CI 1.8-9.1)和转氨酶>2ULN(OR 2.6,95%CI 1.3-6.7)与严重 SARS-CoV-2 独立相关。FIB-4<1.45 是保护因素(OR 0.42,95%CI 0.23-0.76)。肝脂肪变性对疾病过程没有影响。代谢改变的存在与严重 SARS-CoV-2 感染相关,并存的合并症越多,疾病严重程度的风险越高。正常的 FIB-4 值与严重的 SARS-CoV-2 呈负相关,无论是否存在代谢合并症,这提示可以使用这些值来分层严重感染的风险。