Diaz-Soto Maria P, Garcia-Tsao Guadalupe
Hospital Medicine Unit, Massachusetts General Hospital, Boston, MA, USA.
Section of Digestive Diseases, Yale School of Medicine, PO Box 208056, 333 Cedar Street, LMP 1080, New Haven, CT 06520-8019, USA.
Therap Adv Gastroenterol. 2022 Jun 20;15:17562848221101712. doi: 10.1177/17562848221101712. eCollection 2022.
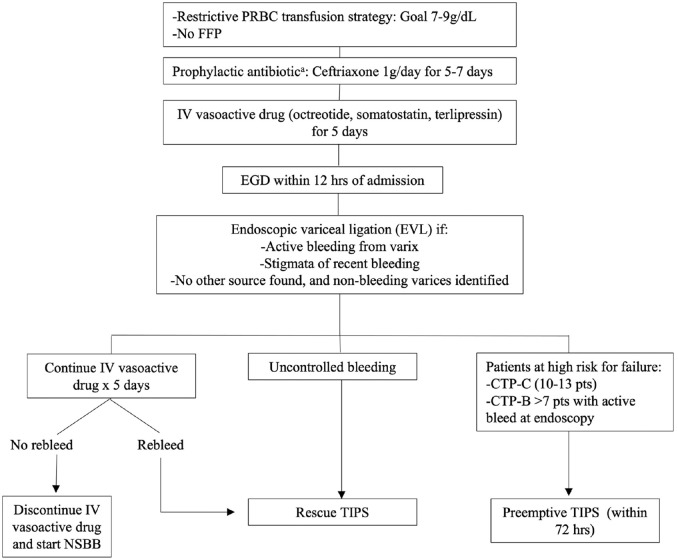
Cirrhosis consists of two main stages: compensated (asymptomatic) and decompensated, the latter with a higher mortality. Variceal hemorrhage, together with ascites or encephalopathy, or both, are events that define cirrhosis decompensation and are driven by portal hypertension. The approach and management of patients with compensated cirrhosis has been mostly focused on preventing variceal hemorrhage in those who have high-risk varices on endoscopy. Recent studies suggest a paradigm shift aimed at preventing all decompensating events, not only variceal hemorrhage, in patients with cirrhosis and clinically significant portal hypertension identified noninvasive measures such as liver stiffness and platelet count. In these patients, nonselective beta-blockers have been shown to prevent ascites (the most common decompensating event) and variceal growth. Variceal hemorrhage has a high mortality rate and even though advances in diagnostic approach and standard of care over the past decades have led to a decrease in mortality, it is still high with a 6-week mortality rate of 15-20%. Survival has improved with the preemptive placement of the transjugular intrahepatic portosystemic shunt in patients at high risk of failing standard therapy. In this review, we provide an overview of the pathophysiology and bases for therapy of portal hypertension and varices, the diagnostic approach and management of compensated cirrhosis with clinically significant portal hypertension, and the management of acute variceal hemorrhage as well as prevention strategies for variceal hemorrhage recurrence.
代偿期(无症状)和失代偿期,后者死亡率更高。静脉曲张破裂出血,以及腹水或肝性脑病,或两者同时出现,是定义肝硬化失代偿的事件,由门静脉高压驱动。代偿期肝硬化患者的治疗方法和管理主要集中在内镜检查发现有高危静脉曲张的患者中预防静脉曲张破裂出血。最近的研究表明,对于通过肝硬度和血小板计数等非侵入性措施确定的肝硬化和具有临床显著门静脉高压的患者,治疗范式发生了转变,旨在预防所有失代偿事件,而不仅仅是静脉曲张破裂出血。在这些患者中,已证明非选择性β受体阻滞剂可预防腹水(最常见的失代偿事件)和静脉曲张生长。静脉曲张破裂出血的死亡率很高,尽管过去几十年诊断方法和治疗标准的进步导致死亡率有所下降,但仍然很高,6周死亡率为15%-20%。对于标准治疗失败风险高的患者,经颈静脉肝内门体分流术的预防性放置改善了生存率。在本综述中,我们概述了门静脉高压和静脉曲张的病理生理学及治疗基础、具有临床显著门静脉高压的代偿期肝硬化的诊断方法和管理,以及急性静脉曲张破裂出血的管理以及静脉曲张破裂出血复发的预防策略。