Department of Respiratory Medicine, Kanagawa Cardiovascular and Respiratory Center, Yokohama, Kanagawa, Japan.
Department of Thoracic Oncology, Kanagawa Cancer Center, Yokohama, Kanagawa, Japan.
Oncologist. 2022 Sep 2;27(9):720-e702. doi: 10.1093/oncolo/oyac118.
Interstitial pneumonia (IP) is a poor prognostic comorbidity in patients with non-small cell lung cancer (NSCLC) and is also a risk factor for pneumonitis. The TORG1936/AMBITIOUS trial, the first known phase II study of atezolizumab in patients with NSCLC with comorbid IP, was terminated early because of the high incidence of severe pneumonitis.
This study included patients with idiopathic chronic fibrotic IP, with a predicted forced vital capacity (%FVC) of >70%, with or without honeycomb lung, who had previously been treated for NSCLC. The patients received atezolizumab every 3 weeks. The primary endpoint was the 1-year survival rate.
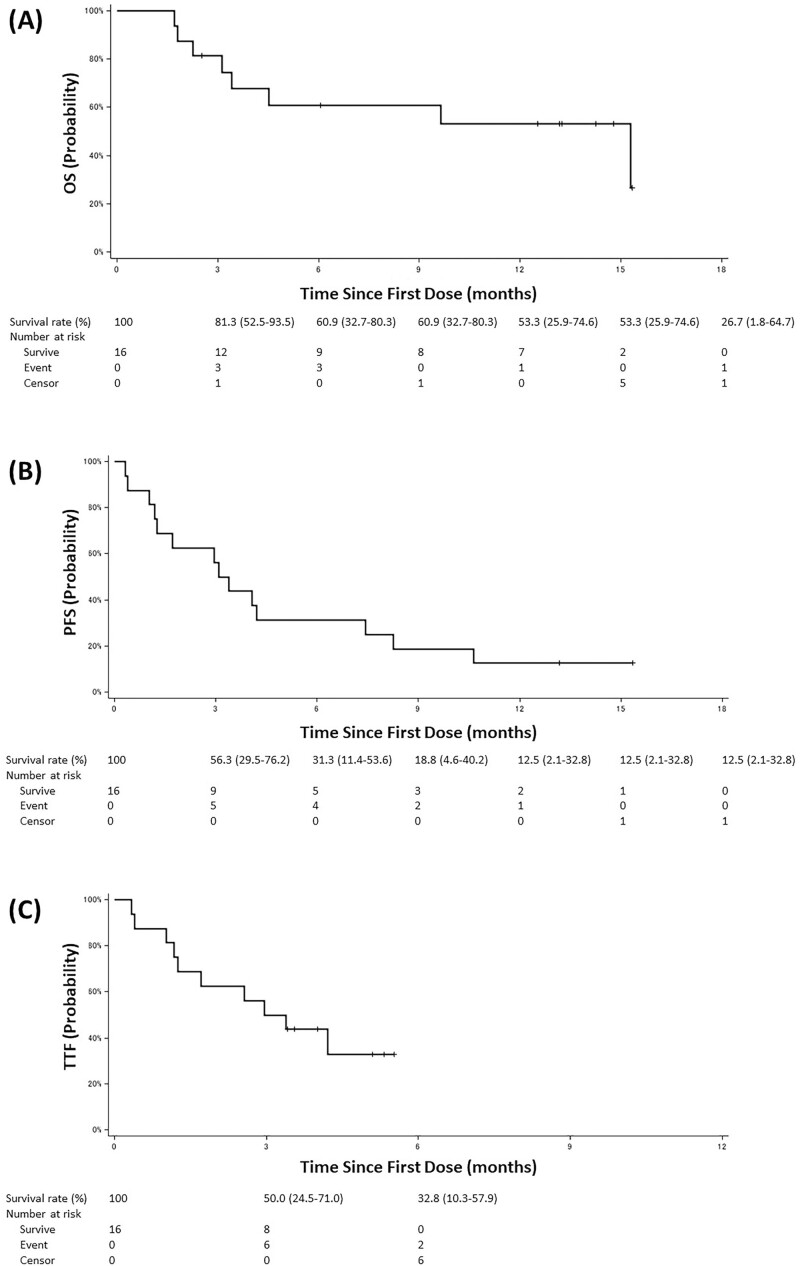
A total of 17 patients were registered; the median %FVC was 85.4%, and 41.2% had honeycomb lungs. The 1-year survival rate was 53.3% (95% CI, 25.9-74.6). The median overall and progression-free survival times were 15.3 months (95% CI, 3.1-not reached) and 3.2 months (95% CI, 1.2-7.4), respectively. The incidence of pneumonitis was 29.4% for all grades, and 23.5% for grade ≥3. Tumor mutational burden and any of the detected somatic mutations were not associated with efficacy or risk of pneumonitis.
Atezolizumab may be one of the treatment options for patients with NSCLC with comorbid IP, despite the high risk of developing pneumonitis. This clinical trial was retrospectively registered in the Japan Registry of Clinical Trials on August 26, 2019, (registry number: jRCTs031190084, https://jrct.niph.go.jp/en-latest-detail/jRCTs031190084).
间质性肺炎(IP)是非小细胞肺癌(NSCLC)患者预后不良的合并症,也是肺炎的危险因素。TORG1936/AMBITIOUS 试验是第一项已知的在合并有 IP 的 NSCLC 患者中使用阿特珠单抗的 II 期研究,由于严重肺炎的发生率较高,该试验提前终止。
本研究纳入了特发性慢性纤维化 IP 患者,这些患者预计用力肺活量(%FVC)>70%,无论是否存在蜂窝肺,且曾接受过 NSCLC 治疗。患者每 3 周接受一次阿特珠单抗治疗。主要终点是 1 年生存率。
共登记了 17 例患者;中位 %FVC 为 85.4%,41.2%有蜂窝肺。1 年生存率为 53.3%(95%CI,25.9-74.6)。中位总生存期和无进展生存期分别为 15.3 个月(95%CI,3.1-未达到)和 3.2 个月(95%CI,1.2-7.4)。所有等级的肺炎发生率为 29.4%,≥3 级的肺炎发生率为 23.5%。肿瘤突变负担和任何检测到的体细胞突变与疗效或肺炎风险无关。
尽管发生肺炎的风险较高,但阿特珠单抗可能是合并有 IP 的 NSCLC 患者的治疗选择之一。本临床试验于 2019 年 8 月 26 日在日本临床试验注册中心(注册号:jRCTs031190084,https://jrct.niph.go.jp/en-latest-detail/jRCTs031190084)进行了回顾性注册。