The Cardiovascular Department, Chang Gung Memorial Hospital, Linkou, Taoyuan, 33305, Taiwan.
College of Medicine, Chang Gung University, Taoyuan City, 33302, Taiwan.
Cardiovasc Diabetol. 2022 Jun 28;21(1):118. doi: 10.1186/s12933-022-01549-x.
Although a few meta-analyses were conducted to compare the risk of incident atrial fibrillation (AF) between sodium-glucose cotransporter-2 inhibitor (SGLT2i), glucagon-like peptide-1 receptor agonists (GLP-1RA), and other anti-hyperglycemic agents using indirect or direct comparison, the above analyses showed conflicting results with each other. We aimed to evaluate the risk of new-onset AF associated with the use of SGLT2i, GLP-1RA, and dipeptidyl peptidase-4 inhibitor (DPP4i) among a large longitudinal cohort of diabetic patients.
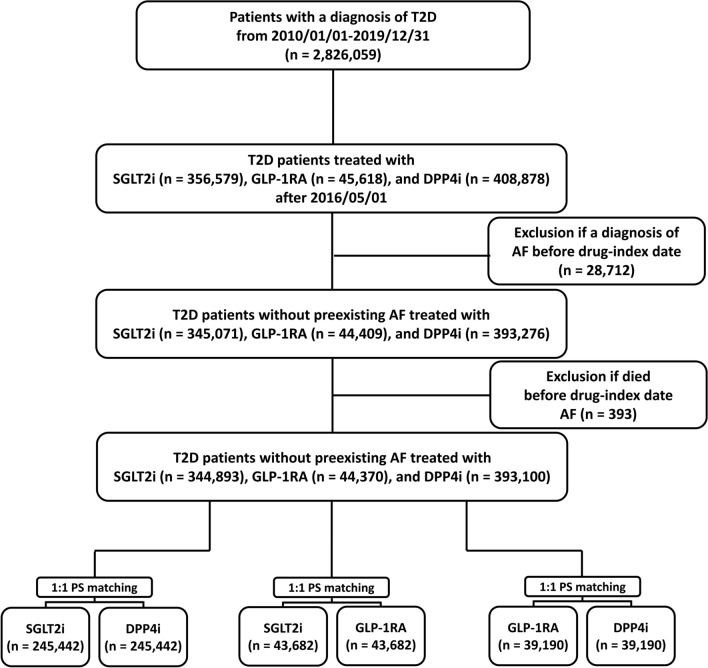
In this nationwide retrospective cohort study based on the Taiwan National Health Insurance Research Database, a total of 344,893, 44,370, and 393,100 consecutive patients with type 2 diabetes without preexisting AF receiving GLP-1RA, SGLT2i, and DPP4i, respectively, were enrolled from May 1, 2016, to December 31, 2019. We used 1:1 propensity score matching (PSM) to balance covariates across paired study groups. Patients were followed from the drug index date until the occurrence of AF, death, discontinuation of the index drug, or the end of the study period (December 31, 2020), whichever occurred first.
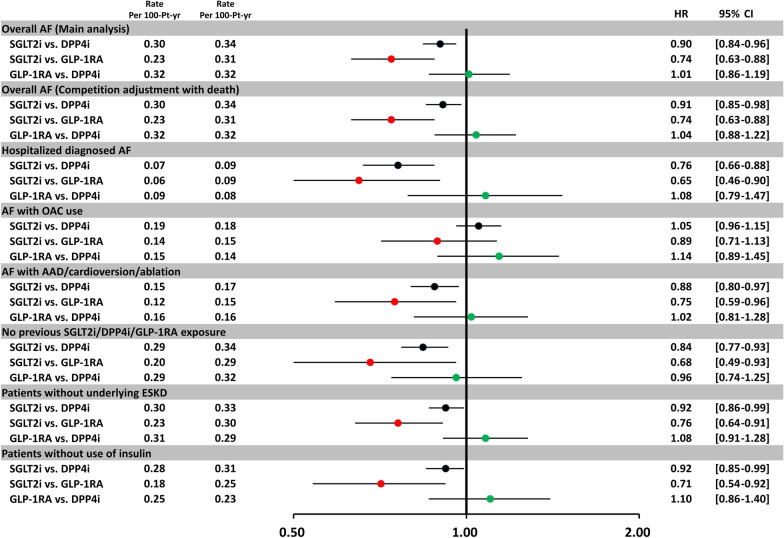
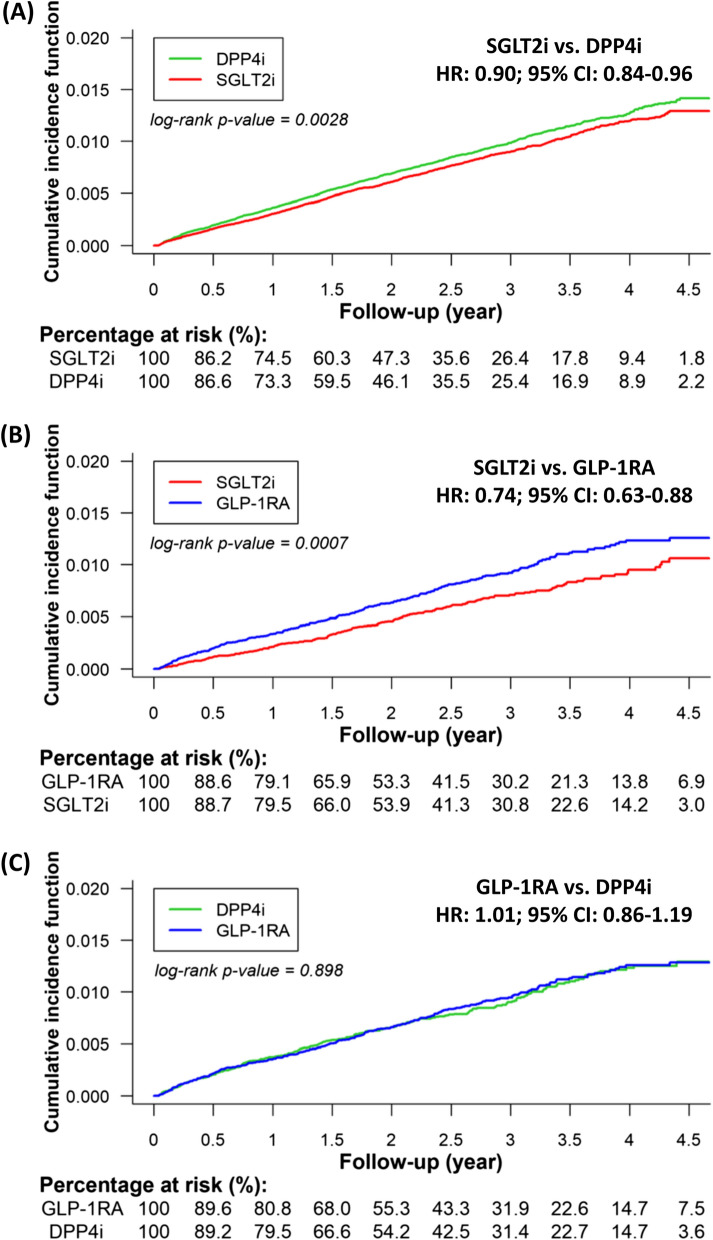
After PSM, there were 245,442, 43,682, and 39,190 paired cohorts of SGLT2i-DPP4i, SGLT2i-GLP-1RA, and GLP-1RA-DPP4i, respectively. SGLT2i treatment was associated with lower risk of new-onset AF in participants with type 2 diabetes compared with either DPP4i [hazard ratio (HR):0.90; 95% confidential interval (CI) 0.84-0.96; P = 0.0028] or GLP-1RA [HR 0.74; 95% CI 0.63-0.88; P = 0.0007] treatment after PSM. There was no difference in the risk of incident AF between GLP-1RA and DPP4i users [HR 1.01; 95% CI 0.86-1.19; P = 0.8980]. The above findings persisted among several important subgroups. Dapagliflozin was specifically associated with a lower risk of new-onset AF compared with DPP4i (P interaction = 0.02).
Compared with DPP4i, SGLT2i but not GLP-1RA was associated with a lower risk of incident AF in patients with type 2 diabetes.
尽管已有几项荟萃分析比较了钠-葡萄糖共转运蛋白 2 抑制剂(SGLT2i)、胰高血糖素样肽-1 受体激动剂(GLP-1RA)和其他抗高血糖药物治疗 2 型糖尿病患者时新发心房颤动(AF)的风险,这些分析采用间接或直接比较,但彼此之间的结果相互矛盾。我们旨在评估在使用 SGLT2i、GLP-1RA 和二肽基肽酶-4 抑制剂(DPP4i)的大型纵向糖尿病患者队列中,新发生 AF 与 SGLT2i、GLP-1RA 和 DPP4i 相关的风险。
本研究基于台湾全民健康保险研究数据库,采用全国性回顾性队列研究,于 2016 年 5 月 1 日至 2019 年 12 月 31 日,纳入分别接受 GLP-1RA、SGLT2i 和 DPP4i 的无预先存在的 AF 的 344893、44370 和 393100 例连续 2 型糖尿病患者。我们使用 1:1 倾向评分匹配(PSM)来平衡配对研究组之间的协变量。从药物索引日期开始,患者将一直随访,直至发生 AF、死亡、索引药物停药或研究结束(2020 年 12 月 31 日),以先发生者为准。
PSM 后,SGLT2i-DPP4i、SGLT2i-GLP-1RA 和 GLP-1RA-DPP4i 配对队列分别有 245442、43682 和 39190 对。与 DPP4i 相比,SGLT2i 治疗与 2 型糖尿病患者新发 AF 的风险较低[风险比(HR):0.90;95%置信区间(CI)0.84-0.96;P=0.0028]或 GLP-1RA[HR 0.74;95% CI 0.63-0.88;P=0.0007]治疗。GLP-1RA 和 DPP4i 使用者发生 AF 的风险无差异[HR 1.01;95% CI 0.86-1.19;P=0.8980]。在几个重要的亚组中,上述发现仍然存在。与 DPP4i 相比,达格列净与新发 AF 风险降低相关(P 交互=0.02)。
与 DPP4i 相比,SGLT2i 而非 GLP-1RA 与 2 型糖尿病患者新发 AF 风险降低相关。