Padmapriyadarsini Chandrasekaran, Vohra Vikram, Bhatnagar Anuj, Solanki Rajesh, Sridhar Rathinam, Anande Lalitkumar, Muthuvijaylakshmi M, Bhatia Miraa, Jeyadeepa Bharathi, Taneja Gaurav, Balaji S, Shah Prashant, Saravanan N, Chauhan Vijay, Kumar Hemanth, Ponnuraja Chinnayin, Livchits Viktoriya, Bahl Monica, Alavadi Umesh, Sachdeva K S, Swaminathan Soumya
ICMR-National Institute for Research in Tuberculosis, Chennai, India.
National Institute for Tuberculosis and Respiratory Diseases, New Delhi, India.
Clin Infect Dis. 2022 Jun 29;76(3):e938-46. doi: 10.1093/cid/ciac528.
Treatment success rates for multidrug-resistant tuberculosis (MDR-TB) remain low globally. Availability of newer drugs has given scope to develop regimens that can be patient-friendly, less toxic, with improved outcomes. We proposed to determine the effectiveness of an entirely oral, short-course regimen with Bedaquiline and Delamanid in treating MDR-TB with additional resistance to fluoroquinolones (MDR-TBFQ+) or second-line injectable (MDR-TBSLI+).
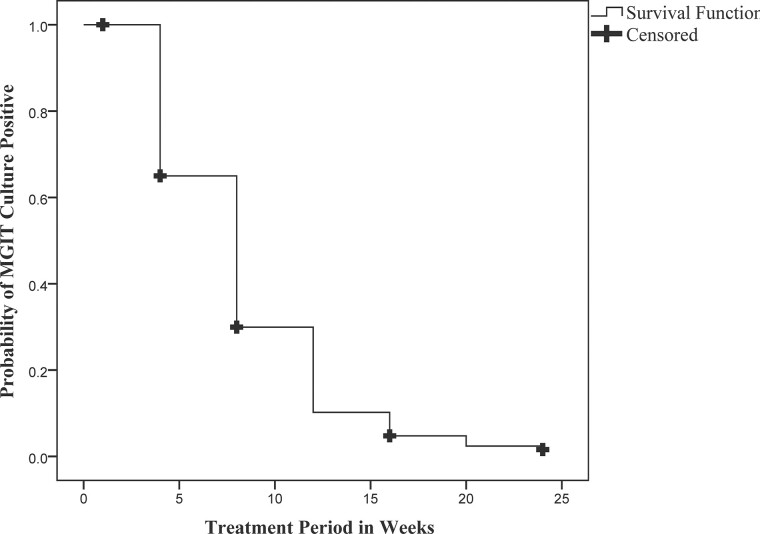
We prospectively determined the effectiveness and safety of combining two new drugs with two repurposed drugs - Bedaquiline, Delamanid, Linezolid, and Clofazimine for 24-36 weeks in adults with pulmonary MDR-TBFQ+ or/and MDR-TBSLI+. The primary outcome was a favorable response at end of treatment, defined as two consecutive negative cultures taken four weeks apart. The unfavorable outcomes included bacteriologic or clinical failure during treatment period.
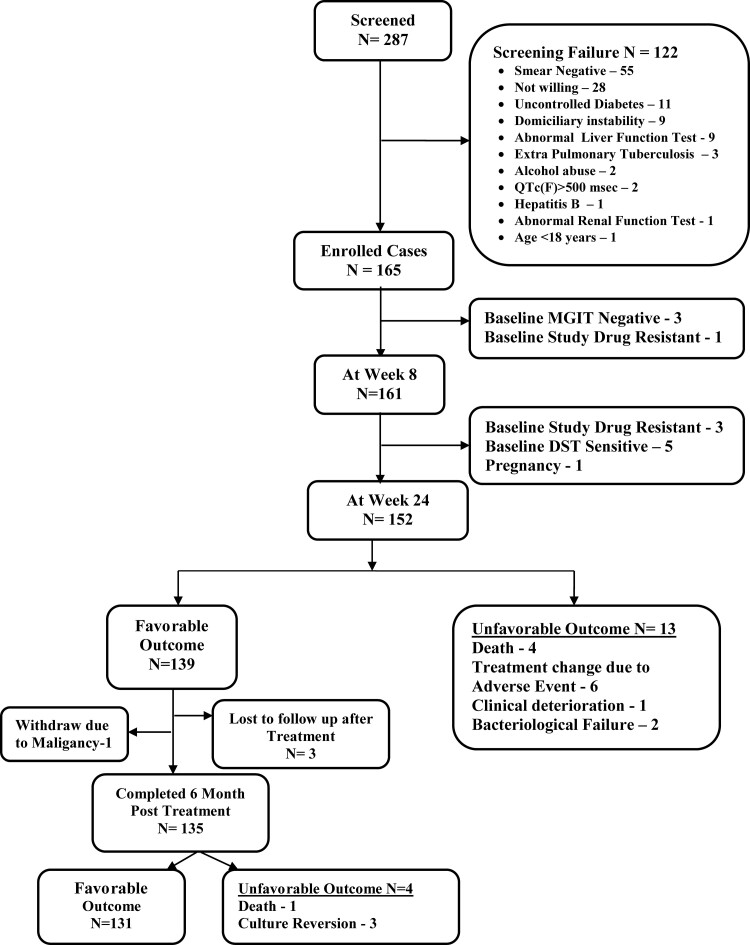
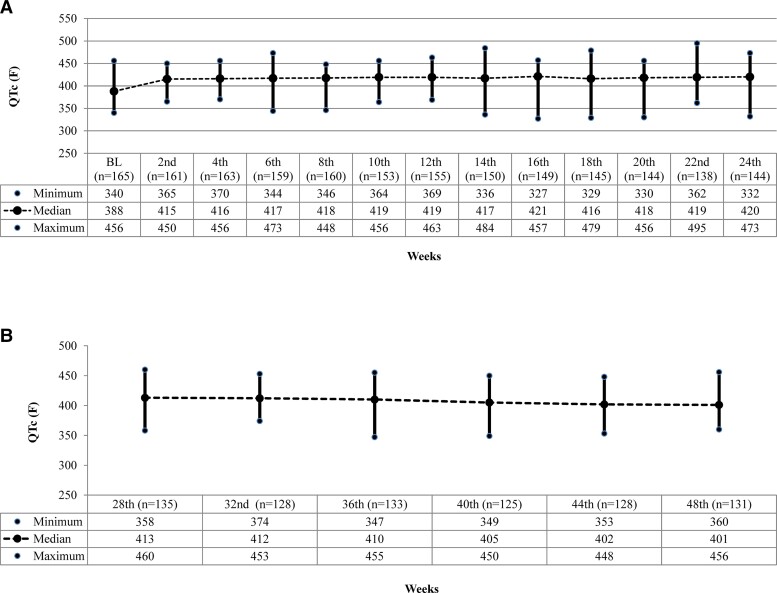
Of the 165 participants enrolled, 158 had MDR-TBFQ+. At the end of treatment, after excluding 12 patients due to baseline drug susceptibility and culture negatives, 139 of 153 patients (91%) had a favorable outcome. Fourteen patients (9%) had unfavorable outcomes: four deaths, seven treatment changes, two bacteriological failures, and one withdrawal. During treatment, 85 patients (52%) developed myelosuppression, 69 (42%) reported peripheral neuropathy, and none had QTc(F) prolongation >500msec. At 48 weeks of follow-up, 131 patients showed sustained treatment success with the resolution of adverse events in the majority.
After 24-36 weeks of treatment, this regimen resulted in a satisfactory favorable outcome in pulmonary MDR-TB patients with additional drug resistance. Cardiotoxicity was minimal, and myelosuppression, while common, was detected early and treated successfully.
全球耐多药结核病(MDR-TB)的治疗成功率仍然很低。新型药物的出现为开发对患者友好、毒性较小且疗效更佳的治疗方案提供了空间。我们提议确定一种含贝达喹啉和地拉曼德的全口服短程治疗方案治疗对氟喹诺酮类药物有额外耐药性(MDR-TBFQ+)或对二线注射剂有额外耐药性(MDR-TBSLI+)的耐多药结核病的有效性。
我们前瞻性地确定了将两种新药与两种重新利用的药物——贝达喹啉、地拉曼德、利奈唑胺和氯法齐明联合使用24至36周对患有肺部MDR-TBFQ+或/和MDR-TBSLI+的成人的有效性和安全性。主要结局是治疗结束时的良好反应,定义为相隔四周采集的连续两次培养阴性。不良结局包括治疗期间的细菌学或临床失败。
在纳入的165名参与者中,158名患有MDR-TBFQ+。治疗结束时,在排除12名因基线药物敏感性和培养阴性的患者后,153名患者中的139名(91%)有良好结局。14名患者(9%)有不良结局:4例死亡、7例治疗方案变更、2例细菌学失败和1例退出。治疗期间,85名患者(52%)出现骨髓抑制,69名(42%)报告有周围神经病变,且无QTc(F)延长>500毫秒。在随访48周时,131名患者显示持续治疗成功,大多数不良事件得到缓解。
经过24至36周的治疗,该方案在患有额外耐药性的肺部耐多药结核病患者中产生了令人满意的良好结局。心脏毒性极小,骨髓抑制虽然常见,但能早期发现并成功治疗。