Division of Radiation Oncology, Vetsuisse Faculty, University of Zurich, Zurich, Switzerland.
Department of Physics, University of Zurich, Zurich, Switzerland.
J Vet Intern Med. 2022 Jul;36(4):1353-1364. doi: 10.1111/jvim.16472. Epub 2022 Jun 30.
Local progression of intracranial tumors can be the consequence of insufficient radiation dose delivered. Dose increases in the brain must be made carefully so as not to risk debilitating adverse effects such as radiation necrosis.
A new protocol with 10 × 4 Gy + 11% physical dose increase limited to the macroscopic tumor volume results in a clinically better outcome compared to a 10 × 4 Gy protocol.
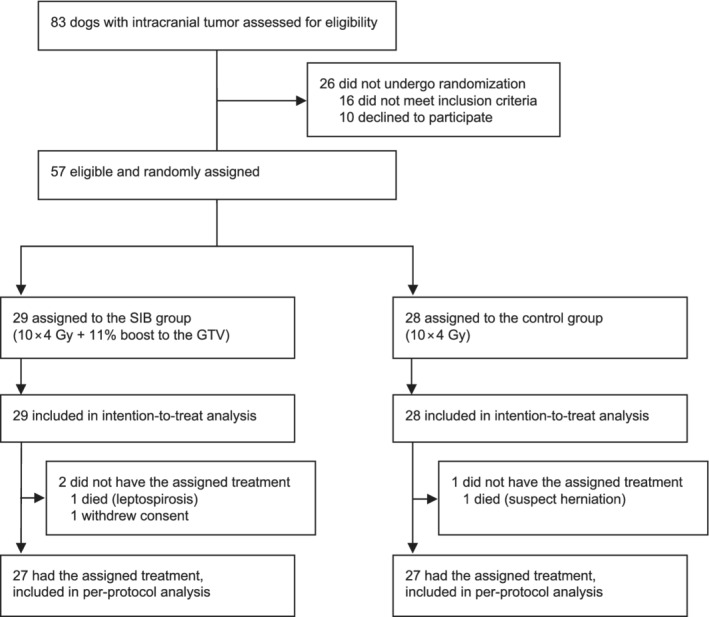
Fifty-seven client-owned dogs with primary intracranial neoplasia.
Randomized controlled trial. Twenty-eight dogs were assigned to the control protocol (10 × 4 Gy) and 29 to the simultaneous integrated boost (SIB) protocol with 4.45 Gy dose increase. Treatment groups were compared for outcome and signs of toxicity.
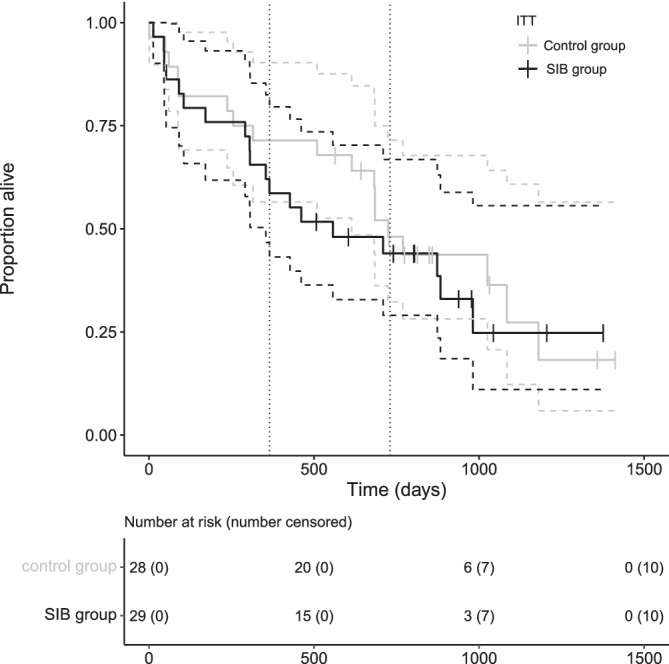
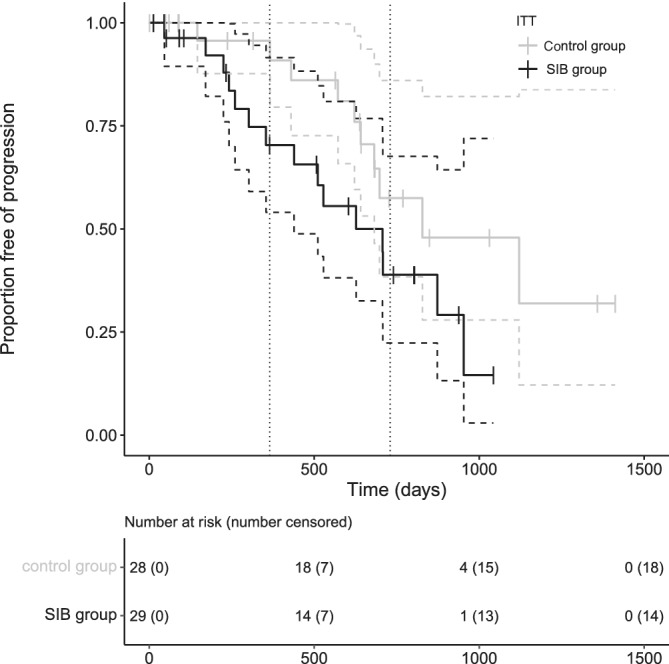
Mild, transient acute or early-delayed adverse radiation effects were observed in 5 dogs. Severe late adverse effects were not seen. Between the protocols, no significant differences were found for outcome (intention-to-treat analysis): overall time to progression (TTP) was 708 days (95% confidence interval (95% CI) [545,872]), in the control group it was 828 days (95% CI [401,1256]), and in the SIB group 627 days (95% CI [282,973]; P = .07). Median overall survival (OS) was 684 days (95% CI [516,853]), in the control group it was 724 days (95% CI [623,826]), and in the SIB group 557 days (95% CI [95,1020]; P = .47). None of the tested variables was prognostic in terms of outcome.
The dose escalation used with an 11% physical dose increase did not result in better outcome.
颅内肿瘤的局部进展可能是由于辐射剂量不足导致的。在大脑中增加剂量必须谨慎,以免造成放射性坏死等致残的不良反应。
与 10×4 Gy 方案相比,一种新的方案,即 10×4 Gy+11%的物理剂量增加,仅限于宏观肿瘤体积,可带来更好的临床结果。
57 只患有原发性颅内肿瘤的患犬。
随机对照试验。28 只狗被分配到对照组(10×4 Gy),29 只狗被分配到同时整合增敏(SIB)组,剂量增加 4.45 Gy。比较两组的治疗结果和毒性体征。
5 只狗出现轻微、短暂的急性或早期迟发性放射性不良反应。未见严重的晚期不良反应。在这两种方案中,对于治疗结果(意向治疗分析),没有发现显著差异:总进展时间(TTP)分别为对照组 708 天(95%置信区间(95%CI)[545,872]),SIB 组 627 天(95%CI[282,973]);P=0.07)。总生存(OS)中位数分别为对照组 684 天(95%CI[516,853]),SIB 组 557 天(95%CI[95,1020]);P=0.47)。在预后方面,没有一个测试变量具有统计学意义。
使用 11%的物理剂量增加并未带来更好的结果。