Department of Surgery and Cancer, Gynecologic Oncology, Imperial College London, London, United Kingdom.
Institute of Cancer and Genomic Sciences, University of Birmingham, Birmingham, United Kingdom.
Am J Obstet Gynecol. 2022 Nov;227(5):735.e1-735.e25. doi: 10.1016/j.ajog.2022.06.052. Epub 2022 Jun 30.
The CovidSurg-Cancer Consortium aimed to explore the impact of COVID-19 in surgical patients and services for solid cancers at the start of the pandemic. The CovidSurg-Gynecologic Oncology Cancer subgroup was particularly concerned about the magnitude of adverse outcomes caused by the disrupted surgical gynecologic cancer care during the COVID-19 pandemic, which are currently unclear.
This study aimed to evaluate the changes in care and short-term outcomes of surgical patients with gynecologic cancers during the COVID-19 pandemic. We hypothesized that the COVID-19 pandemic had led to a delay in surgical cancer care, especially in patients who required more extensive surgery, and such delay had an impact on cancer outcomes.
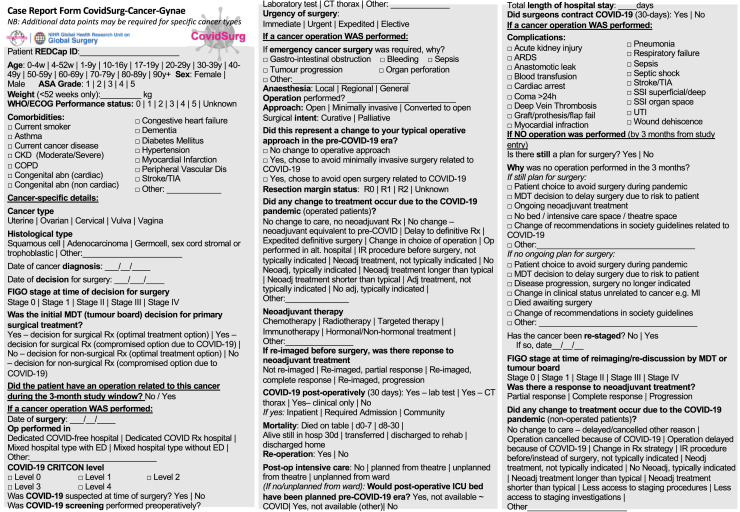
This was a multicenter, international, prospective cohort study. Consecutive patients with gynecologic cancers who were initially planned for nonpalliative surgery, were recruited from the date of first COVID-19-related admission in each participating center for 3 months. The follow-up period was 3 months from the time of the multidisciplinary tumor board decision to operate. The primary outcome of this analysis is the incidence of pandemic-related changes in care. The secondary outcomes included 30-day perioperative mortality and morbidity and a composite outcome of unresectable disease or disease progression, emergency surgery, and death.
We included 3973 patients (3784 operated and 189 nonoperated) from 227 centers in 52 countries and 7 world regions who were initially planned to have cancer surgery. In 20.7% (823/3973) of the patients, the standard of care was adjusted. A significant delay (>8 weeks) was observed in 11.2% (424/3784) of patients, particularly in those with ovarian cancer (213/1355; 15.7%; P<.0001). This delay was associated with a composite of adverse outcomes, including disease progression and death (95/424; 22.4% vs 601/3360; 17.9%; P=.024) compared with those who had operations within 8 weeks of tumor board decisions. One in 13 (189/2430; 7.9%) did not receive their planned operations, in whom 1 in 20 (5/189; 2.7%) died and 1 in 5 (34/189; 18%) experienced disease progression or death within 3 months of multidisciplinary team board decision for surgery. Only 22 of the 3778 surgical patients (0.6%) acquired perioperative SARS-CoV-2 infections; they had a longer postoperative stay (median 8.5 vs 4 days; P<.0001), higher predefined surgical morbidity (14/22; 63.6% vs 717/3762; 19.1%; P<.0001) and mortality (4/22; 18.2% vs 26/3762; 0.7%; P<.0001) rates than the uninfected cohort.
One in 5 surgical patients with gynecologic cancer worldwide experienced management modifications during the COVID-19 pandemic. Significant adverse outcomes were observed in those with delayed or cancelled operations, and coordinated mitigating strategies are urgently needed.
CovidSurg-癌症联合会旨在探讨大流行开始时 COVID-19 对接受实体癌症手术治疗的患者和服务的影响。CovidSurg-妇科肿瘤癌症亚组特别关注 COVID-19 大流行期间手术妇科癌症护理中断所导致的不良后果的严重程度,目前尚不清楚。
本研究旨在评估 COVID-19 大流行期间接受妇科癌症手术治疗的患者的护理和短期结局的变化。我们假设 COVID-19 大流行导致了癌症护理的延迟,特别是对于需要更广泛手术的患者,并且这种延迟对癌症结局产生了影响。
这是一项多中心、国际性、前瞻性队列研究。从每个参与中心首次与 COVID-19 相关入院之日起,连续招募了最初计划进行非姑息性手术的妇科癌症患者,招募时间为 3 个月。随访期为多学科肿瘤委员会决定手术之日起 3 个月。本分析的主要结局是与大流行相关的护理变化的发生率。次要结局包括 30 天围手术期死亡率和发病率以及不可切除疾病或疾病进展、急诊手术和死亡的复合结局。
我们纳入了来自全球 52 个国家和 7 个世界地区的 227 个中心的 3973 名患者(3784 名接受手术和 189 名未接受手术),这些患者最初计划接受癌症手术。在 20.7%(823/3973)的患者中,调整了标准治疗方案。在 11.2%(424/3784)的患者中观察到显著延迟(>8 周),尤其是卵巢癌患者(213/1355;15.7%;P<.0001)。与在肿瘤委员会决定后 8 周内接受手术的患者相比,这种延迟与包括疾病进展和死亡在内的不良结局复合结局相关(95/424;22.4% vs. 601/3360;17.9%;P=.024)。13 名患者中有 1 名(189/2430;7.9%)未接受计划手术,其中 1/20(5/189;2.7%)死亡,1/5(34/189;18%)在多学科团队决定手术后 3 个月内经历疾病进展或死亡。在 3778 名接受手术的患者中,只有 22 名(0.6%)发生围手术期 SARS-CoV-2 感染;他们的术后住院时间更长(中位数 8.5 天 vs. 4 天;P<.0001),术前定义的手术发病率更高(14/22;63.6% vs. 717/3762;19.1%;P<.0001)和死亡率(4/22;18.2% vs. 26/3762;0.7%;P<.0001)比未感染组高。
全球范围内每 5 名接受妇科癌症手术治疗的患者中就有 1 名经历了治疗管理的改变。对于接受延迟或取消手术的患者,观察到了显著的不良后果,迫切需要协调缓解策略。