Department of Anesthesiology and Critical Care, University of Pennsylvania, Philadelphia, PA, 19104, USA.
Leonard Davis Institute for Health Economics, Philadelphia, PA, 19104, USA.
BMC Health Serv Res. 2022 Jul 2;22(1):855. doi: 10.1186/s12913-022-08251-4.
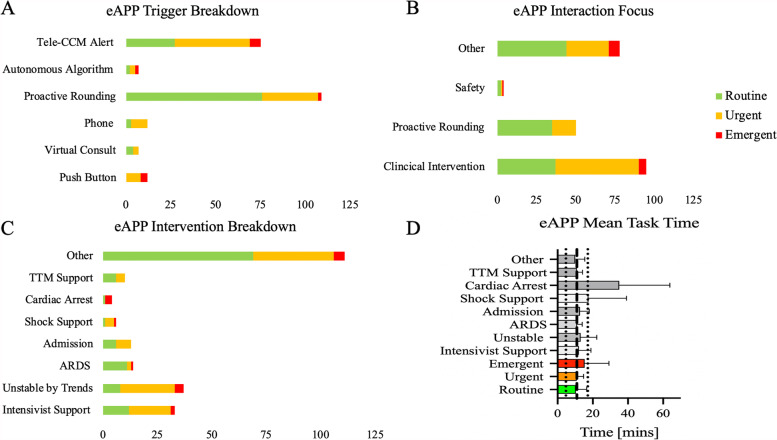
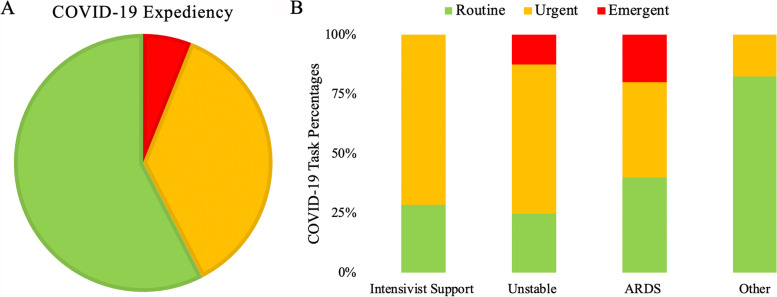
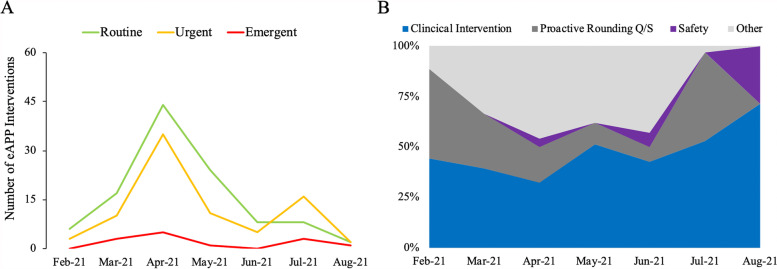
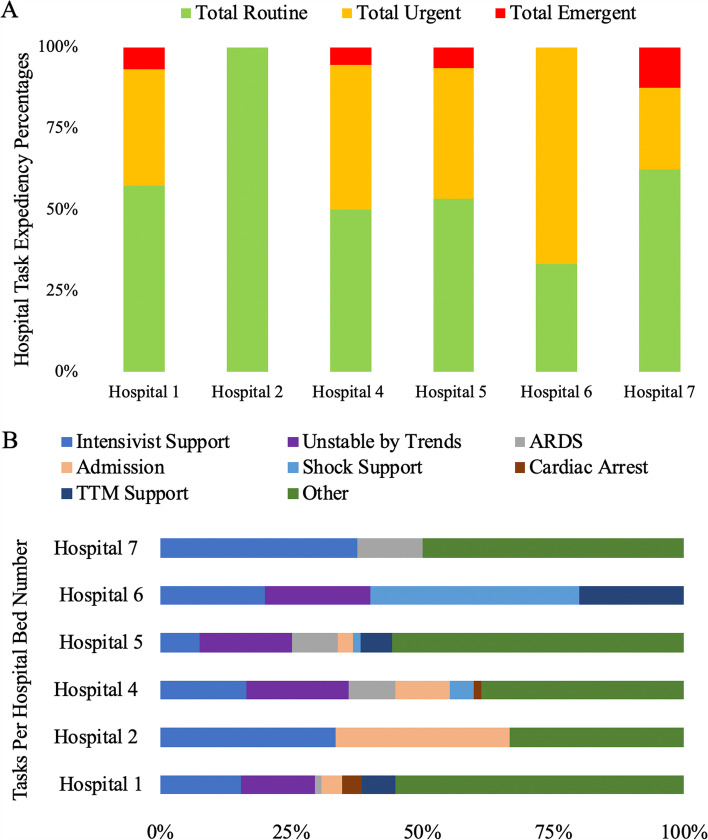
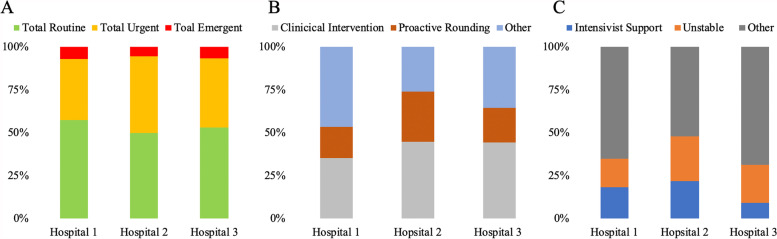
Incorporating the advanced practice provider (APP) in the delivery of tele critical care medicine (teleCCM) addresses the critical care provider shortage. However, the current literature lacks details of potential workflows, deployment difficulties and implementation outcomes while suggesting that expanding teleCCM service may be difficult. Here, we demonstrate the implementation of a telemedicine APP (eAPP) pilot service within an existing teleCCM program with the objective of determining the feasibility and ease of deployment. The goal is to augment an existing tele-ICU system with a balanced APP service to assess the feasibility and potential impact on the ICU performance in several hospitals affiliated within a large academic center. A REDCap survey was used to assess eAPP workflows, expediency of interventions, duration of tasks, and types of assignments within different service locations. Between 02/01/2021 and 08/31/2021, 204 interventions (across 133 12-h shift) were recorded by eAPP (n = 109 (53.4%); n = 82 (40.2%); n = 13 (6.4%). The average task duration was 10.9 ± 6.22 min, but there was a significant difference based on the expediency of the task (F [2; 202] = 3.89; p < 0.022) and type of tasks (F [7; 220] = 6.69; p < 0.001). Furthermore, the eAPP task type and expediency varied depending upon the unit engaged and timeframe since implementation. The eAPP interventions were effectively communicated with bedside staff with only 0.5% of suggestions rejected. Only in 2% cases did the eAPP report distress. In summary, the eAPP can be rapidly deployed in existing teleCCM settings, providing adaptable and valuable care that addresses the specific needs of different ICUs while simultaneously enhancing the delivery of ICU care. Further studies are needed to quantify the input more robustly.
将高级实践提供者(APP)纳入远程危重病医学(teleCCM)的实施有助于解决危重病提供者短缺的问题。然而,目前的文献缺乏有关潜在工作流程、部署困难和实施结果的详细信息,同时表明扩大 teleCCM 服务可能很困难。在这里,我们展示了在现有的 teleCCM 计划中实施远程医疗 APP(eAPP)试点服务,目的是确定可行性和部署的容易程度。目标是通过平衡的 APP 服务来增强现有的远程 ICU 系统,以评估在隶属于一个大型学术中心的几家医院中的 ICU 性能的可行性和潜在影响。使用 REDCap 调查来评估 eAPP 工作流程、干预的及时性、任务的持续时间以及在不同服务地点的任务类型。在 2021 年 2 月 1 日至 2021 年 8 月 31 日期间,eAPP 记录了 204 次干预措施(分布在 133 个 12 小时班次中)(n=109(53.4%);n=82(40.2%);n=13(6.4%)。平均任务持续时间为 10.9±6.22 分钟,但根据任务的及时性(F[2;202]=3.89;p<0.022)和任务类型(F[7;220]=6.69;p<0.001)存在显著差异。此外,eAPP 的任务类型和及时性取决于参与的单位和实施以来的时间框架。eAPP 干预措施与床边工作人员有效沟通,只有 0.5%的建议被拒绝。只有在 2%的情况下,eAPP 报告了困境。总之,eAPP 可以快速部署在现有的 teleCCM 环境中,提供适应性强且有价值的护理,满足不同 ICU 的特定需求,同时增强 ICU 护理的提供。需要进一步的研究来更有力地量化投入。