Laubach Markus, Suresh Sinduja, Herath Buddhi, Wille Marie-Luise, Delbrück Heide, Alabdulrahman Hatem, Hutmacher Dietmar W, Hildebrand Frank
Department of Orthopaedics, Trauma and Reconstructive Surgery, RWTH Aachen University Hospital, Pauwelsstraße 30, 52074, Aachen, Germany.
Australian Research Council (ARC) Training Centre for Multiscale 3D Imaging, Modelling, and Manufacturing (M3D Innovation), Queensland University of Technology, Brisbane, QLD, 4000, Australia.
J Orthop Translat. 2022 Jun 16;34:73-84. doi: 10.1016/j.jot.2022.04.004. eCollection 2022 May.
Bone defects after trauma, infection, or tumour resection present a challenge for patients and clinicians. To date, autologous bone graft (ABG) is the gold standard for bone regeneration. To address the limitations of ABG such as limited harvest volume as well as overly fast remodelling and resorption, a new treatment strategy of scaffold-guided bone regeneration (SGBR) was developed. In a well-characterized sheep model of large to extra-large tibial segmental defects, three-dimensional (3D) printed composite scaffolds have shown clinically relevant biocompatibility and osteoconductive capacity in SGBR strategies. Here, we report four challenging clinical cases with large complex posttraumatic long bone defects using patient-specific SGBR as a successful treatment.
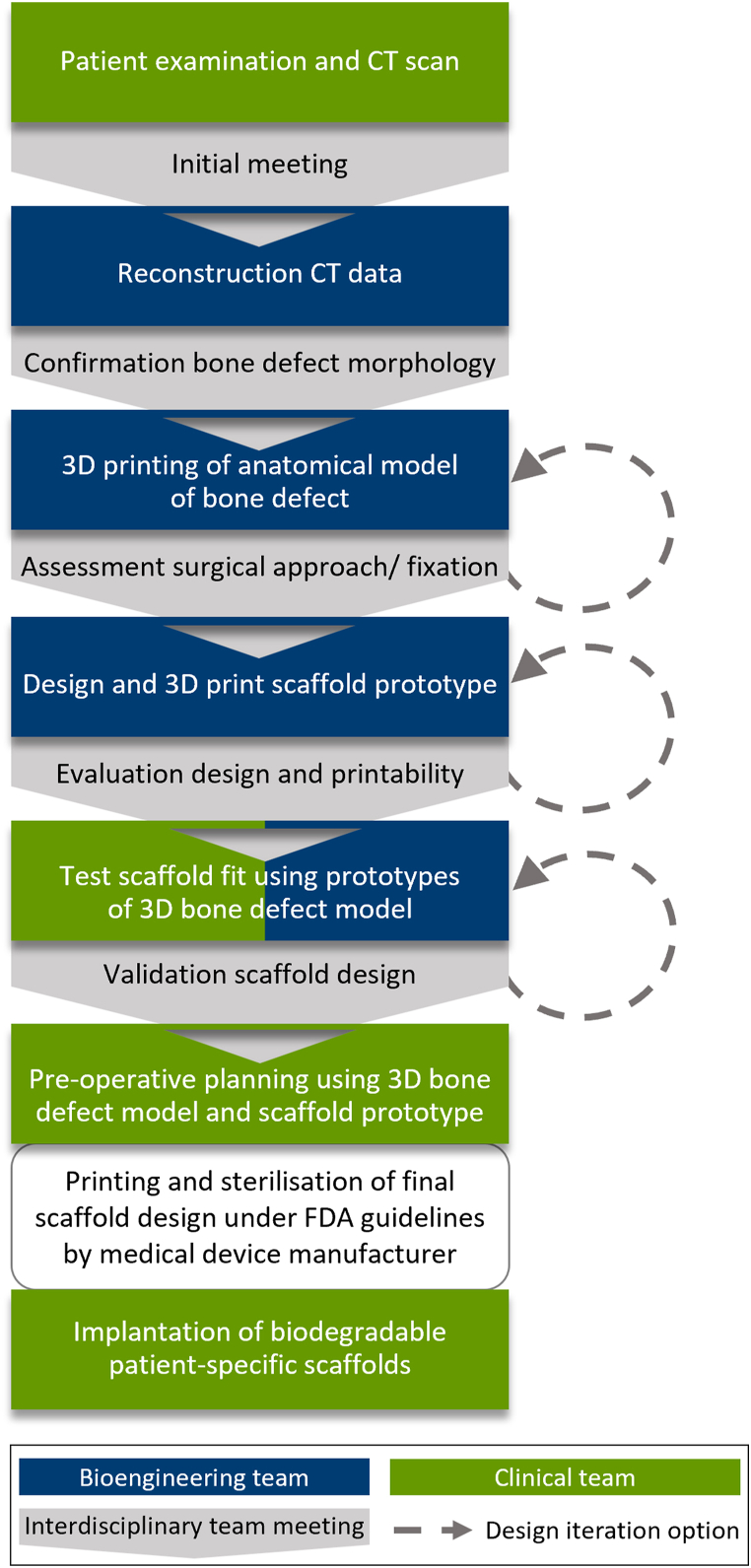
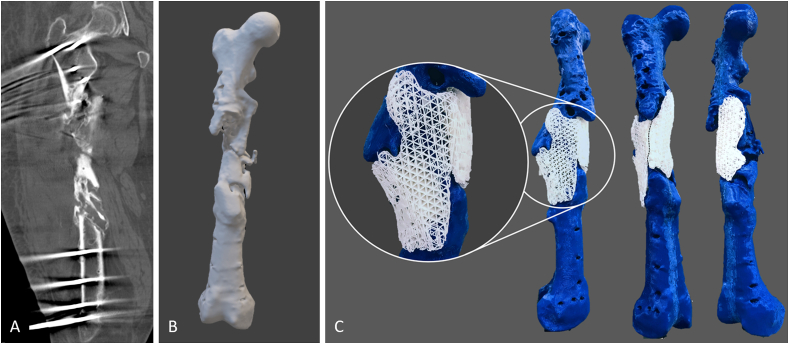
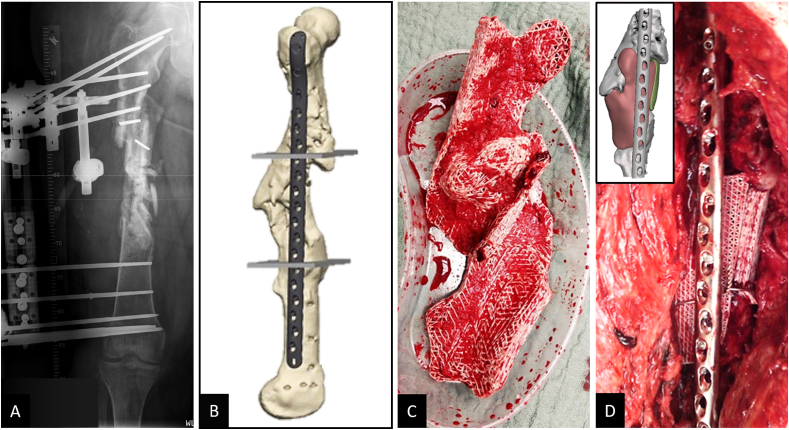
After giving informed consent computed tomography (CT) images were used to design patient-specific biodegradable medical-grade polycaprolactone-tricalcium phosphate (mPCL-TCP, 80:20 wt%) scaffolds. The CT scans were segmented using Materialise Mimics to produce a defect model and the scaffold parts were designed with Autodesk Meshmixer. Scaffold prototypes were 3D-printed to validate robust clinical handling and bone defect fit. The final scaffold design was additively manufactured under Food and Drug Administration (FDA) guidelines for patient-specific and custom-made implants by Osteopore International Pte Ltd.
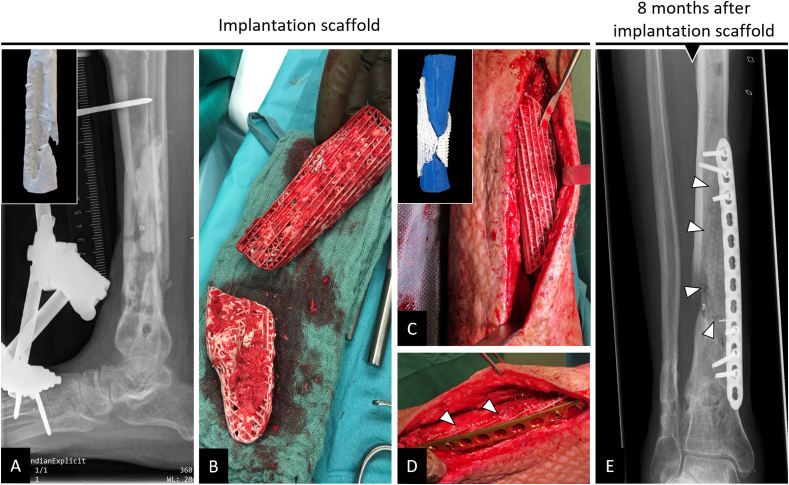
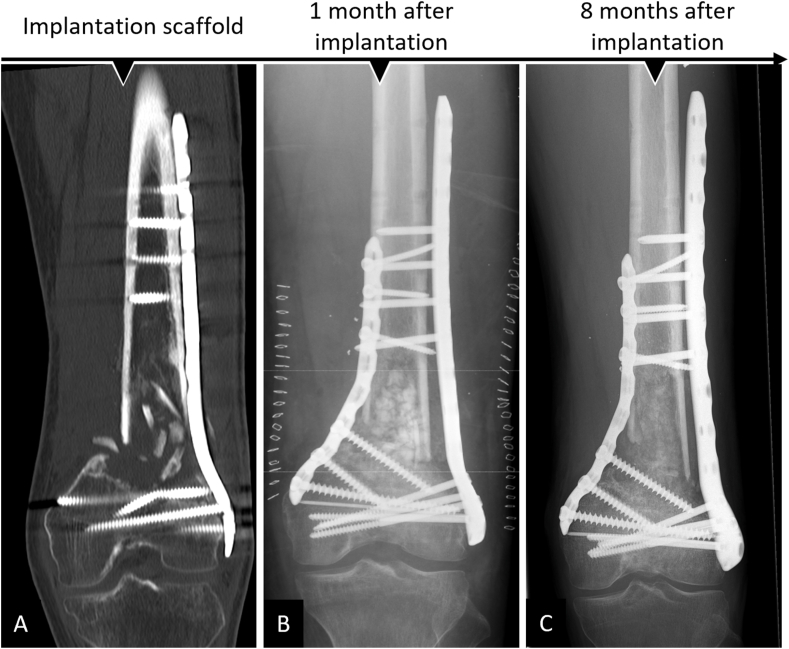
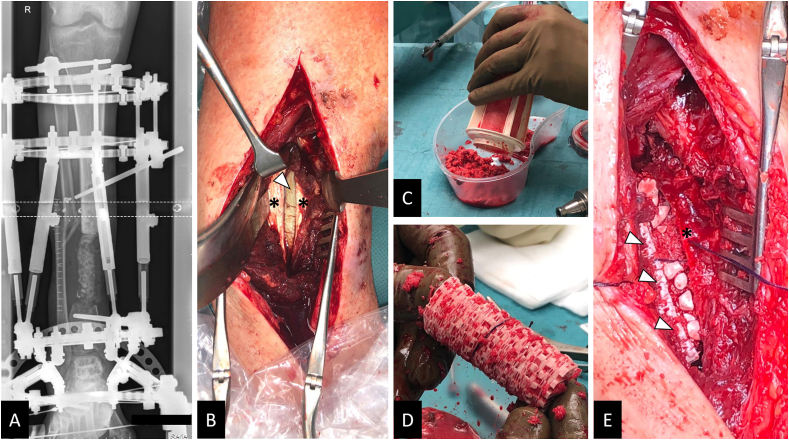
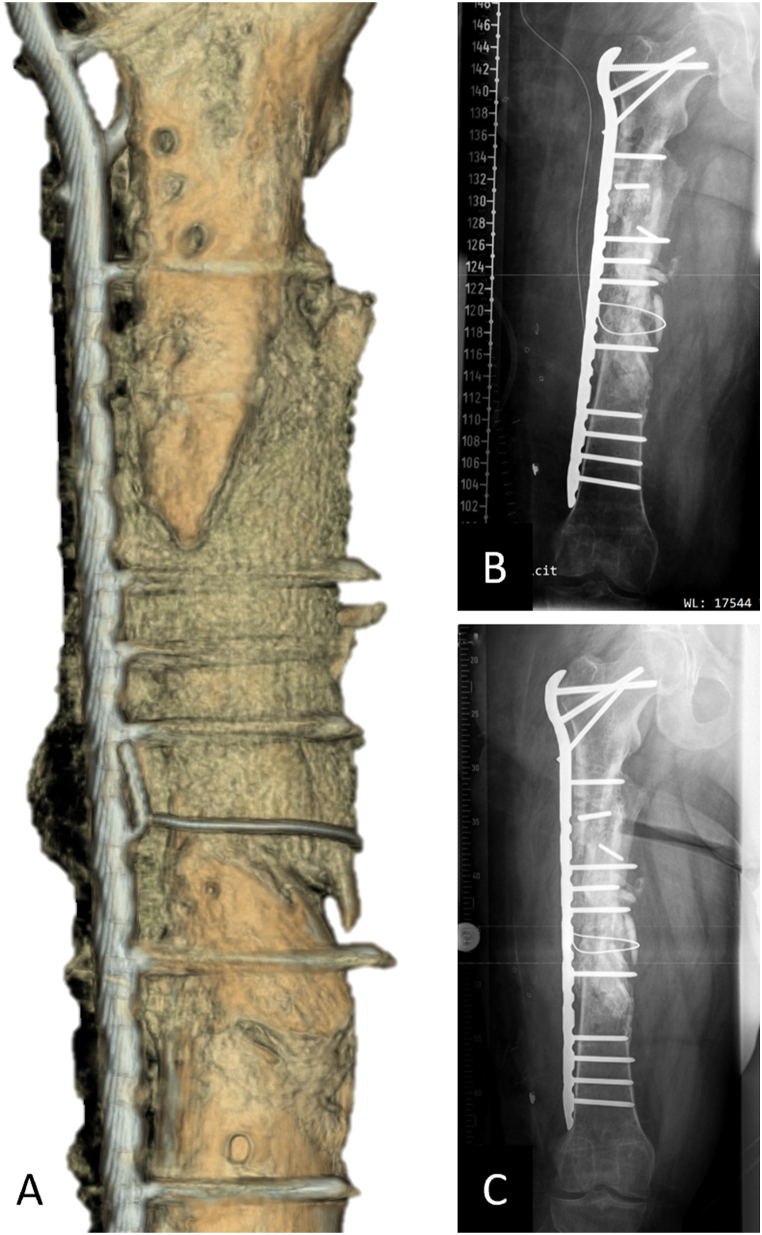
Four patients (age: 23-42 years) with posttraumatic lower extremity large long bone defects (case 1: 4 cm distal femur, case 2: 10 cm tibia shaft, case 3: complex malunion femur, case 4: irregularly shaped defect distal tibia) are presented. After giving informed consent, the patients were treated surgically by implanting a custom-made mPCL-TCP scaffold loaded with ABG (case 2: additional application of recombinant human bone morphogenetic protein-2) harvested with the Reamer-Irrigator-Aspirator system (RIA, Synthes®). In all cases, the scaffolds matched the actual anatomical defect well and no perioperative adverse events were observed. Cases 1, 3 and 4 showed evidence of bony ingrowth into the large honeycomb pores (pores >2 mm) and fully interconnected scaffold architecture with indicative osseous bridges at the bony ends on the last radiographic follow-up (8-9 months after implantation). Comprehensive bone regeneration and full weight bearing were achieved in case 2 at follow-up 23 months after implantation.
This study shows the bench to bedside translation of guided bone regeneration principles into scaffold-based bone tissue engineering. The scaffold design in SGBR should have a tissue-specific morphological signature which stimulates and directs the stages from the initial host response towards the full regeneration. Thereby, the scaffolds provide a physical niche with morphology and biomaterial properties that allow cell migration, proliferation, and formation of vascularized tissue in the first one to two months, followed by functional bone formation and the capacity for physiological bone remodelling. Great design flexibility of composite scaffolds to support the one to three-year bone regeneration was observed in four patients with complex long bone defects.
This study reports on the clinical efficacy of SGBR in the treatment of long bone defects. Moreover, it presents a comprehensive narrative of the rationale of this technology, highlighting its potential for bone regeneration treatment regimens in patients with any type of large and complex osseous defects.
创伤、感染或肿瘤切除后的骨缺损给患者和临床医生带来了挑战。迄今为止,自体骨移植(ABG)是骨再生的金标准。为解决ABG的局限性,如收获量有限以及过度快速的重塑和吸收,开发了一种新的支架引导骨再生(SGBR)治疗策略。在一个特征明确的大至超大胫骨节段性缺损绵羊模型中,三维(3D)打印复合支架在SGBR策略中已显示出临床相关的生物相容性和骨传导能力。在此,我们报告了4例具有大型复杂创伤后长骨缺损的具有挑战性的临床病例,使用患者特异性SGBR作为成功的治疗方法。
在获得知情同意后,使用计算机断层扫描(CT)图像设计患者特异性的可生物降解医用级聚己内酯 - 磷酸三钙(mPCL - TCP,80:20 wt%)支架。使用Materialise Mimics对CT扫描进行分割以生成缺损模型,并使用Autodesk Meshmixer设计支架部件。3D打印支架原型以验证稳健的临床操作和骨缺损适配性。最终的支架设计由Osteopore International Pte Ltd根据美国食品药品监督管理局(FDA)针对患者特异性和定制植入物的指南进行增材制造。
呈现了4例患者(年龄:23 - 42岁),均有创伤后下肢大型长骨缺损(病例1:股骨远端4 cm,病例2:胫骨干10 cm,病例3:股骨复杂畸形愈合,病例4:胫骨远端不规则形状缺损)。在获得知情同意后,对患者进行手术治疗,植入加载有ABG的定制mPCL - TCP支架(病例2:额外应用重组人骨形态发生蛋白 - 2),ABG通过扩髓 - 冲洗 - 吸引系统(RIA,Synthes®)获取。在所有病例中,支架与实际解剖缺损匹配良好,未观察到围手术期不良事件。病例1、3和4在最后一次影像学随访(植入后8 - 9个月)时显示有骨长入大蜂窝孔(孔径>2 mm)以及完全相互连接的支架结构,在骨端有指示性骨桥。病例2在植入后23个月的随访中实现了全面的骨再生和完全负重。
本研究展示了从实验台到床边将引导骨再生原理转化为基于支架的骨组织工程。SGBR中的支架设计应具有组织特异性形态特征,可刺激并引导从初始宿主反应到完全再生的各个阶段。因此,支架提供了一个具有形态和生物材料特性的物理微环境,在最初的一到两个月内允许细胞迁移、增殖并形成血管化组织,随后进行功能性骨形成并具备生理性骨重塑能力。在4例复杂长骨缺损患者中观察到复合支架具有很大的设计灵活性以支持一到三年的骨再生。
本研究报告了SGBR治疗长骨缺损的临床疗效。此外,它全面阐述了该技术的原理,突出了其在治疗任何类型大型复杂骨缺损患者的骨再生治疗方案中的潜力。