Ten Lohuis Caitlin C, Burke Sarah C, Jannuzzo Cooper J, Barker Nicholas A, Chen Edward P, Busse Laurence W
Emory Critical Care Center, Emory Healthcare, Atlanta, GA.
Department of Anesthesiology, Physician Specialists in Anesthesia, Emory Saint Joseph's Hospital, Atlanta, GA.
Crit Care Explor. 2022 May 13;4(5):e0687. doi: 10.1097/CCE.0000000000000687. eCollection 2022 May.
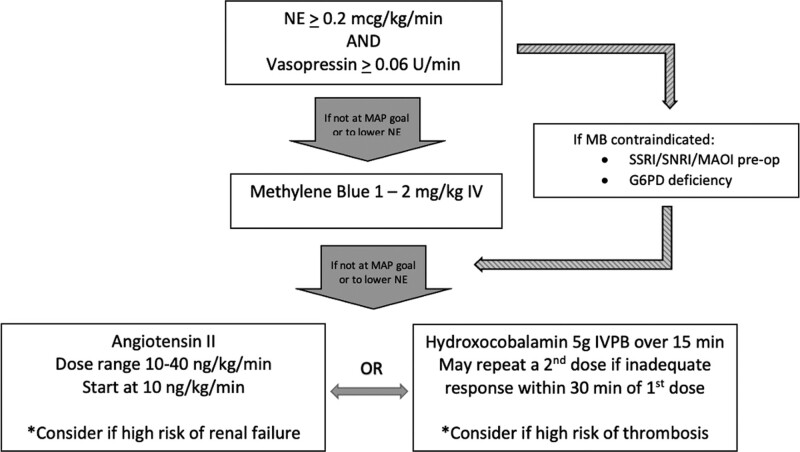
Catecholamines and vasopressin are commonly used in patients with post cardiovascular surgery vasoplegia (PCSV). Multimodal therapy, including methylene blue (MB), hydroxocobalamin, and angiotensin II (Ang II), may improve outcomes in patients who remain hypotensive despite catecholamine and vasopressin therapy. However, a standardized approach has not been established. We created a protocol at Emory Healthcare (Emory Protocol), which provides guidance on norepinephrine equivalent dose (NED) and the use of noncatecholamines in the setting of PCSV and sought to determine the clinical significance of adherence to the protocol.
Retrospective study.
Multisite study at Emory University Hospital.
Patients receiving Ang II for PCSV in any cardiovascular ICU from 2018 to 2020.
Patient encounters were scored on Emory Protocol compliance based on NED (1-5), use of vasopressin (1-2), use of MB (1-2), and documentation of high-output shock (1-4). A compliant score was less than 7, moderately compliant 7 to 8, and poorly compliant greater than 8. Demographics, clinical data, and outcomes were abstracted from the medical records.
Of the 78 consecutive patients receiving Ang II for PCSV, overall ICU mortality was 26.9%, with an average compliance score of 6.2. ICU mortality was 21.1% for compliant cases ( = 38), 29.7% for moderately compliant cases ( = 24), and 37.5% for poorly compliant cases ( = 16). In regression analysis, the cumulative compliance score to the Emory Protocol was predictive of ICU mortality ( = 0.027).
Compliance with the Emory Protocol, emphasizing early initiation of the noncatecholamines vasopressin, MB, hydroxocobalamin, and Ang II at lower catecholamine doses in high-output shock, is associated with improved ICU mortality.
儿茶酚胺和血管加压素常用于心血管手术后血管麻痹(PCSV)患者。多模式治疗,包括亚甲蓝(MB)、羟钴胺素和血管紧张素II(Ang II),可能改善尽管接受儿茶酚胺和血管加压素治疗仍持续低血压的患者的预后。然而,尚未建立标准化方法。我们在埃默里医疗中心制定了一项方案(埃默里方案),该方案提供了关于去甲肾上腺素等效剂量(NED)以及在PCSV情况下使用非儿茶酚胺的指导,并试图确定遵循该方案的临床意义。
回顾性研究。
埃默里大学医院的多中心研究。
2018年至2020年在任何心血管重症监护病房因PCSV接受Ang II治疗的患者。
根据NED(1 - 5)、血管加压素的使用(1 - 2)、MB的使用(1 - 2)以及高输出量休克的记录(1 - 4),对患者的诊疗情况进行埃默里方案依从性评分。依从性评分小于7为依从,7至8为中度依从,大于8为依从性差。从病历中提取人口统计学、临床数据和预后信息。
在连续78例因PCSV接受Ang II治疗的患者中,总体重症监护病房死亡率为26.9%,平均依从性评分为6.2。依从性良好的病例(n = 38)重症监护病房死亡率为21.1%,中度依从的病例(n = 24)为29.7%,依从性差的病例(n = 16)为37.5%。在回归分析中,对埃默里方案的累积依从性评分可预测重症监护病房死亡率(P = 0.027)。
遵循埃默里方案,即在高输出量休克时以较低儿茶酚胺剂量早期启用非儿茶酚胺类药物血管加压素、MB、羟钴胺素和Ang II,与改善重症监护病房死亡率相关。