Gupta Ribhav, Abdalla Safa, Meausoone Valerie, Vicas Nikitha, Mejía-Guevara Iván, Weber Ann M, Cislaghi Beniamino, Darmstadt Gary L
Department of Epidemiology and Population Health, Stanford University School of Medicine, Stanford, CA, USA.
Department of Medicine, University of Minnesota School of Medicine, Minneapolis, MN, USA.
EClinicalMedicine. 2022 Jun 26;50:101513. doi: 10.1016/j.eclinm.2022.101513. eCollection 2022 Aug.
Despite strides towards gender equality, inequalities persist or remain unstudied, due potentially to data gaps. Although mapped, the effects of key data gaps remain unknown. This study provides a framework to measure effects of gender- and age-imbalanced and missing covariate data on gender-health research. The framework is demonstrated using a previously studied pathway for effects of pre-marital sex norms among adults on adolescent HIV risk.
After identifying gender-age-imbalanced Demographic and Health Survey (DHS) datasets, we resampled responses and restricted covariate data from a relatively complete, balanced dataset derived from the 2007 Zambian DHS to replicate imbalanced gender-age sampling and covariate missingness. Differences in model outcomes due to sampling were measured using tests for interaction. Missing covariate effects were measured by comparing fully-adjusted and reduced model fitness.
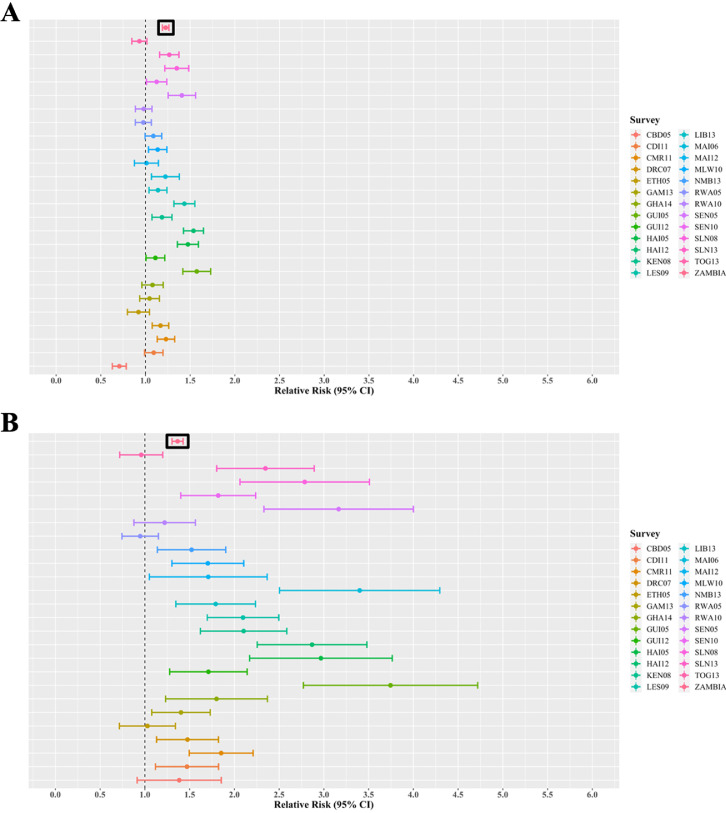
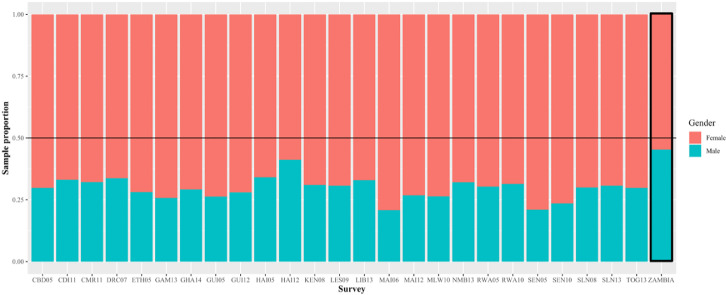
We simulated data from 25 DHS surveys across 20 countries from 2005-2014 on four sex-stratified models for pathways of adult attitude-behaviour discordance regarding pre-marital sex and adolescent risk of HIV. On average, across gender-age-imbalanced surveys, males comprised 29.6% of responses compared to 45.3% in the gender-balanced dataset. Gender-age-imbalanced sampling significantly affected regression coefficients in 40% of model-scenarios ( = 40 of 100) and biased relative-risk estimates away from gender-age-balanced sampling outcomes in 46% ( = 46) of model-scenarios. Model fitness was robust to covariate removal with minor effects on male HIV models. No consistent trends were observed between sampling distribution and risk of biased outcomes.
Gender-health model outcomes may be affected by sampling gender-age-imbalanced data and less-so by missing covariates. Although occasionally attenuated, the effect magnitude of gender-age-imbalanced sampling is variable and may mask true associations, thus misinforming policy dialogue. We recommend future surveys improve balanced gender-age sampling to promote research reliability.
Bill & Melinda Gates Foundation grant OPP1140262 to Stanford University.
尽管在性别平等方面取得了进展,但不平等现象依然存在或尚未得到研究,这可能是由于数据缺口所致。虽然已对关键数据缺口进行了梳理,但其影响仍不明确。本研究提供了一个框架,用于衡量性别和年龄不均衡以及协变量数据缺失对性别与健康研究的影响。该框架通过一条先前研究过的途径得以展示,即成年人婚前性行为规范对青少年感染艾滋病毒风险的影响。
在确定了性别年龄不均衡的人口与健康调查(DHS)数据集后,我们对回复进行了重新抽样,并从2007年赞比亚DHS得出的一个相对完整且平衡的数据集中限制协变量数据,以复制性别年龄不均衡抽样和协变量缺失情况。因抽样导致的模型结果差异通过交互作用检验来衡量。缺失协变量的影响通过比较完全调整模型和简化模型的拟合度来衡量。
我们模拟了2005年至2014年期间20个国家25项DHS调查的数据,用于四个性别分层模型,这些模型涉及成年人在婚前性行为方面态度与行为不一致以及青少年感染艾滋病毒风险的途径。平均而言,在性别年龄不均衡的调查中,男性占回复的29.6%,而在性别平衡的数据集中这一比例为45.3%。性别年龄不均衡抽样在40%的模型情景中(100个情景中的40个)显著影响回归系数,并且在46%(46个)的模型情景中使相对风险估计值偏离性别年龄平衡抽样结果。模型拟合度对协变量去除具有稳健性,对男性艾滋病毒模型影响较小。在抽样分布与有偏差结果的风险之间未观察到一致的趋势。
性别与健康模型结果可能会受到性别年龄不均衡数据抽样的影响,而受协变量缺失的影响较小。尽管有时会减弱,但性别年龄不均衡抽样的影响程度是可变的,可能会掩盖真实关联,从而误导政策对话。我们建议未来的调查改进性别年龄平衡抽样,以提高研究的可靠性。
比尔及梅琳达·盖茨基金会向斯坦福大学提供的OPP1140262号资助。