Jane M. Zhu (
Christina J. Charlesworth, Oregon Health & Science University.
Health Aff (Millwood). 2022 Jul;41(7):1013-1022. doi: 10.1377/hlthaff.2022.00052.
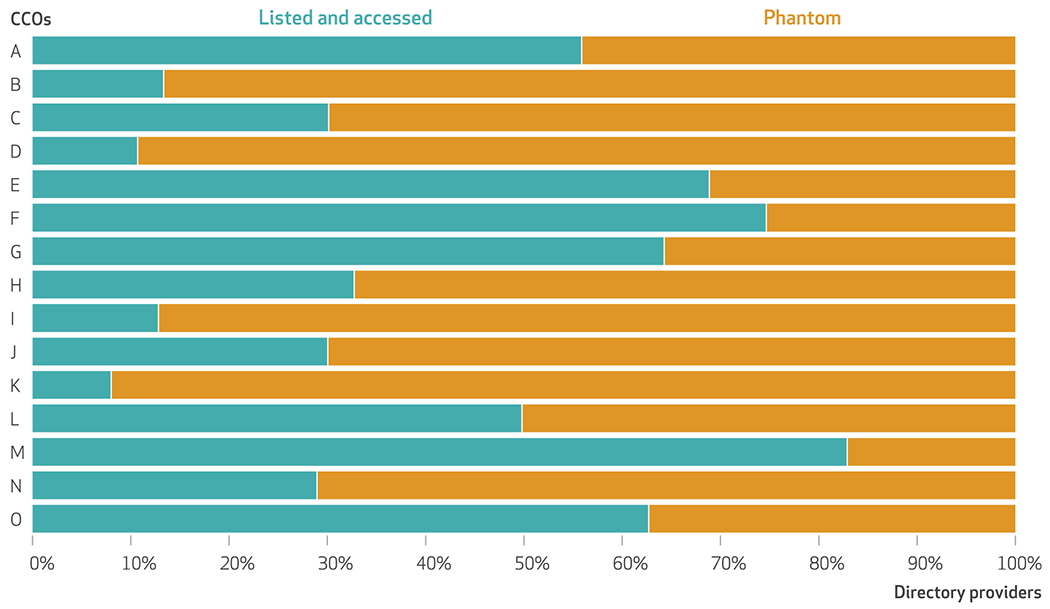
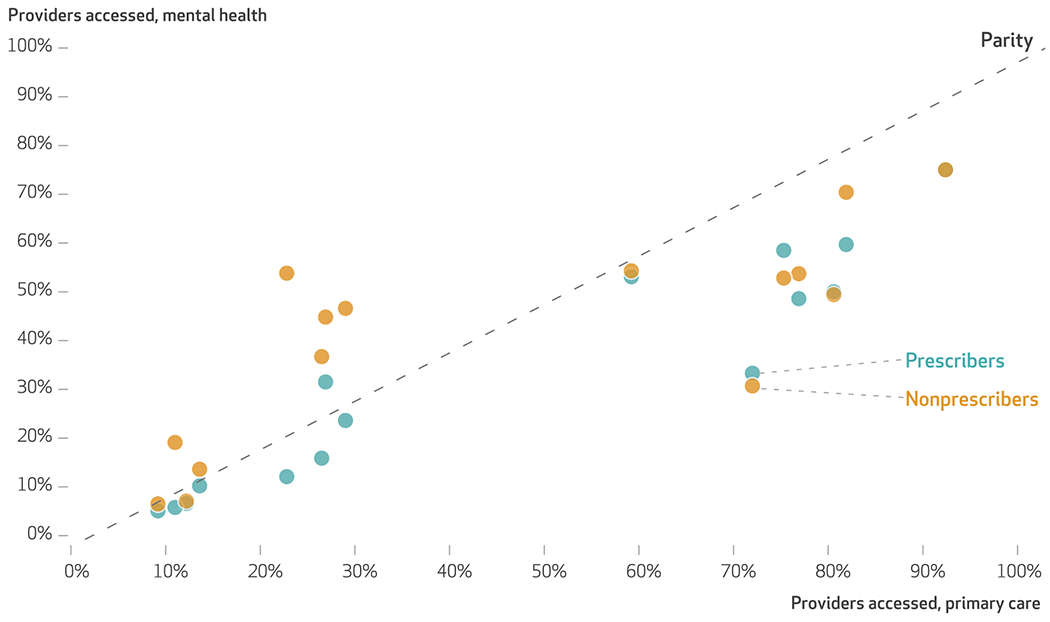
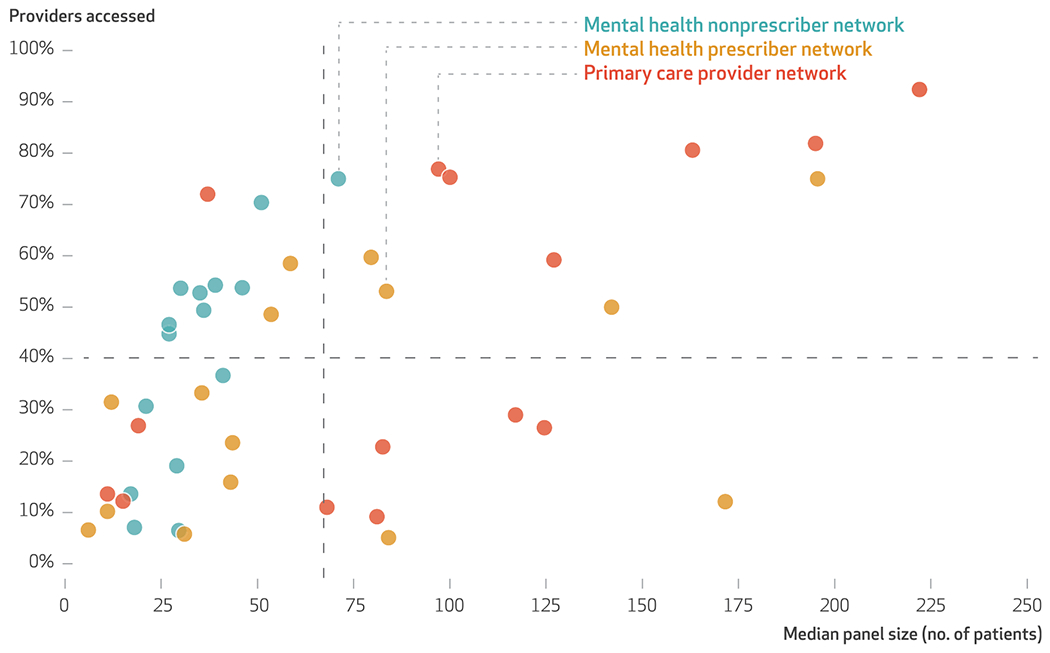
Understanding the extent to which beneficiaries can "realize" access to reported provider networks is imperative in mental health care, where there are significant unmet needs. We compared listings of providers in network directories against provider networks empirically constructed from administrative claims among members who were ages sixty-four and younger and enrolled in Oregon's Medicaid managed care organizations between January 1 and December 31, 2018. "In-network" providers were those with any medical claims filed for at least five unique Medicaid beneficiaries enrolled in a given health plan. They included primary care providers, specialty mental health prescribers, and nonprescribing mental health clinicians. Overall, 58.2 percent of network directory listings were "phantom" providers who did not see Medicaid patients, including 67.4 percent of mental health prescribers, 59.0 percent of mental health nonprescribers, and 54.0 percent of primary care providers. Significant discrepancies between the providers listed in directories and those whom enrollees can access suggest that provider network monitoring and enforcement may fall short if based on directory information.
了解受益人在精神卫生保健方面能够“实际”获得报告的供应商网络的程度至关重要,因为在这方面存在着巨大的未满足需求。我们将网络目录中的供应商清单与从 2018 年 1 月 1 日至 12 月 31 日期间在俄勒冈州医疗补助管理式医疗组织中登记的 64 岁及以下成员的行政索赔中实际构建的供应商网络进行了比较。“网络内”供应商是指至少为五个在特定医疗计划中登记的不同医疗补助受益人的任何医疗索赔进行了报销的供应商。其中包括初级保健提供者、精神科专科处方提供者和非处方精神科临床医生。总体而言,58.2%的网络目录列表是“幻影”供应商,他们不看 Medicaid 患者,包括 67.4%的精神科处方提供者、59.0%的精神科非处方提供者和 54.0%的初级保健提供者。目录中列出的供应商与参保人可获得的供应商之间存在显著差异,这表明如果基于目录信息,供应商网络监测和执行可能会不到位。