Pathology Unit, Azienda Sanitaria Toscana Nord Ovest, Pisa 56121, Italy.
Surgery Unit, Azienda Sanitaria Toscana Nord Ovest, Pisa 56121, Italy.
World J Gastroenterol. 2022 Jun 7;28(21):2396-2402. doi: 10.3748/wjg.v28.i21.2396.
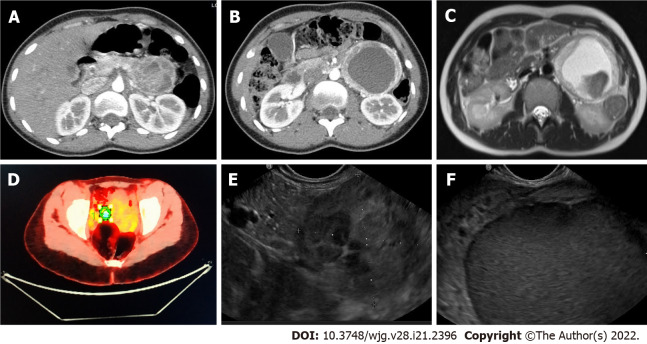
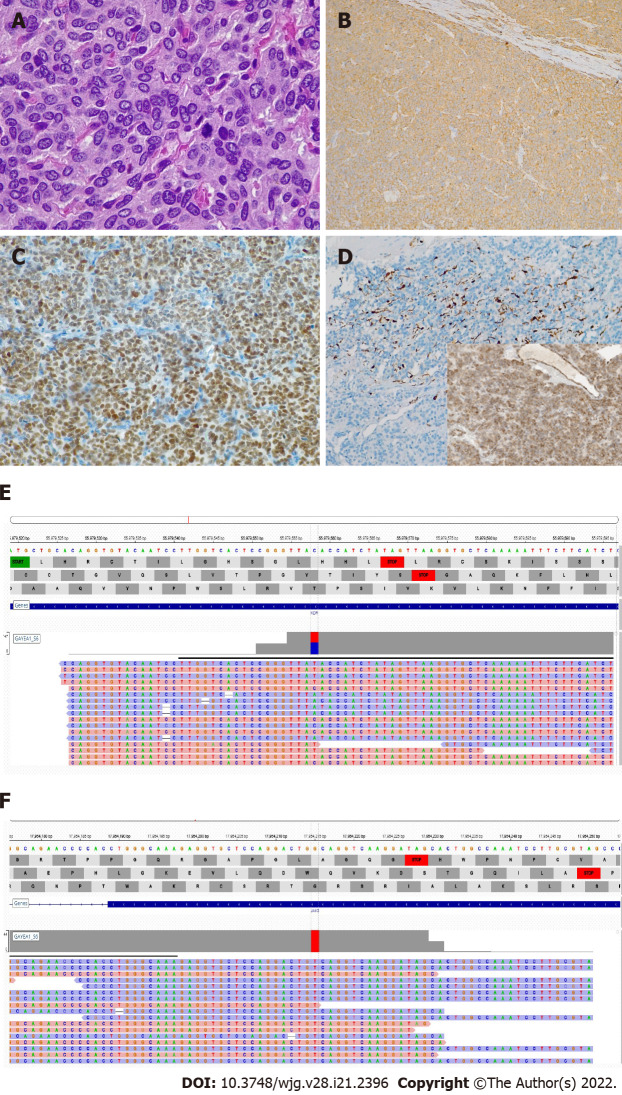
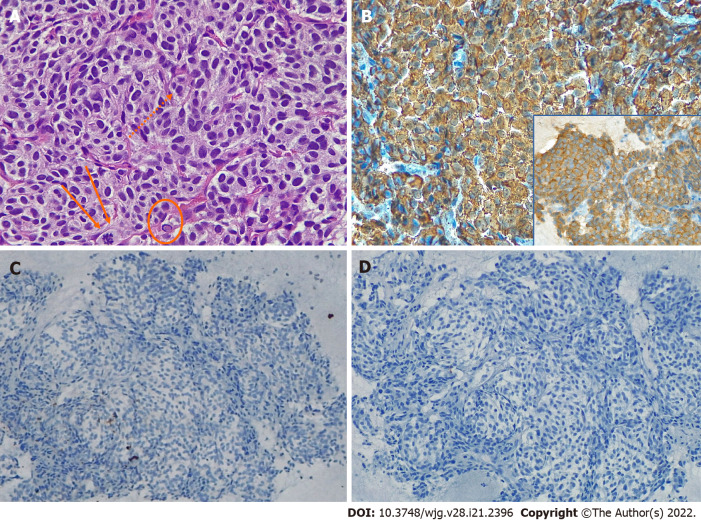
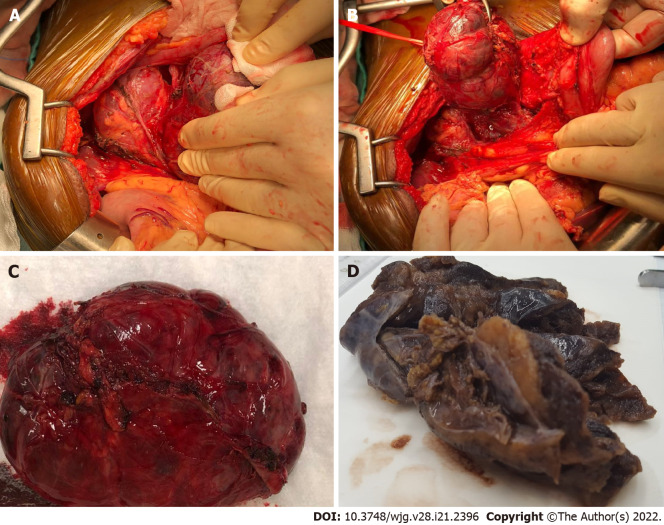
We described the case of a peripancreatic paraganglioma (PGL) misdiagnosed as pancreatic lesion. Surgical exploration revealed an unremarkable pancreas and a large well-defined cystic mass originating at the mesocolon root. Radical enucleation of the mass was performed, preserving the pancreatic tail. Histologically, a diagnosis of PGL was rendered. Interestingly, two previously unreported mutations, one affecting the gene in exon 7 and another on the gene in exon 4 were detected. Both mutations are known to be pathogenetic. Imaging and cytologic findings were blindly reviewed by an expert panel of clinicians, radiologists, and pathologists to identify possible causes of the misdiagnosis. The major issue was lack of evidence of a cleavage plane from the pancreas at imaging, which prompted radiologists to establish an intra-parenchymal origin. The blinded revision shifted the diagnosis towards an extra-pancreatic lesion, as the pancreatic parenchyma showed no structural alterations and no dislocation of the Wirsung duct. , the identified biases were the emergency setting of the radiologic examination and the very thin mesocolon sheet, which hindered clear definition of the lesion borders. Original endoscopic ultrasonography diagnosis was confirmed, emphasizing the intrinsic limit of this technique in detecting large masses. Finally, pathologic review favored a diagnosis of PGL due to the morphological features and immonohistochemical profile. Eighteen months after tumor excision, the patient is asymptomatic with no disease relapse evident by either radiology or laboratory tests. Our report strongly highlights the difficulties in rendering an accurate pre-operative diagnosis of PGL.
我们描述了一例误诊为胰腺病变的胰周副神经节瘤(PGL)。手术探查发现胰腺无明显异常,在横结肠系膜根部有一个大而界限清楚的囊性肿块。对肿块进行了根治性剜除术,保留了胰腺尾部。组织学上,诊断为 PGL。有趣的是,检测到两个以前未报道的突变,一个影响 7 号外显子的 基因,另一个影响 4 号外显子的 基因。这两个突变都被认为是致病的。通过影像学和细胞学检查,由临床医生、放射科医生和病理学家组成的专家组对可能导致误诊的原因进行了盲法审查。主要问题是影像学上缺乏与胰腺分离的证据,这促使放射科医生建立了一个实质内起源的假说。盲法修订后,诊断倾向于胰腺外病变,因为胰腺实质没有结构改变,也没有胰管移位。需要指出的是,导致这种误诊的偏见是放射检查的紧急情况和非常薄的横结肠系膜,这阻碍了病变边界的清晰界定。原始的内镜超声诊断得到了确认,强调了这种技术在检测大肿块方面的固有局限性。最后,病理检查支持 PGL 的诊断,这主要是基于其形态学特征和免疫组织化学特征。肿瘤切除后 18 个月,患者无症状,影像学和实验室检查均未发现疾病复发。我们的报告强烈强调了准确术前诊断 PGL 的困难。