Department of Anesthesiology and Intensive Care, Université Paris-Saclay, Paul Brousse Hospital, Assistance Publique - Hôpitaux de Paris (APHP), Villejuif, France.
Department of Anesthesiology and Perioperative Medicine Sauvegarde Clinic, Ramsay Santé, Lyon, France.
BMC Anesthesiol. 2022 Jul 8;22(1):211. doi: 10.1186/s12871-022-01757-8.
A mismatch between oxygen delivery (DO) and consumption (VO) is associated with increased perioperative morbidity and mortality. Hyperlactatemia is often used as an early screening tool, but this non-continuous measurement requires intermittent arterial line sampling. Having a non-invasive tool to rapidly detect inadequate DO is of great clinical relevance. The respiratory exchange ratio (RER) can be easily measured in all intubated patients and has been shown to predict postoperative complications. We therefore aimed to assess the discriminative ability of the RER to detect an inadequate DO as reflected by hyperlactatemia in patients having intermediate-to-high risk abdominal surgery.
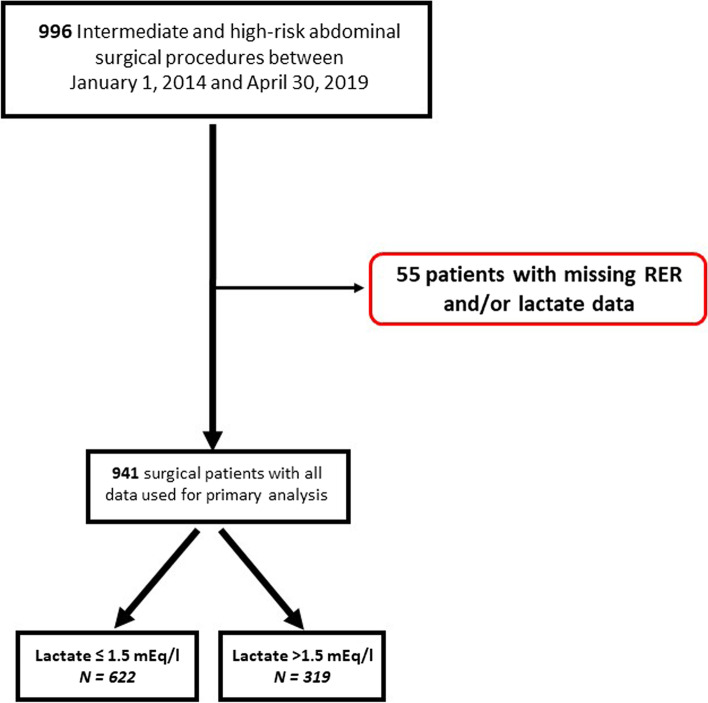
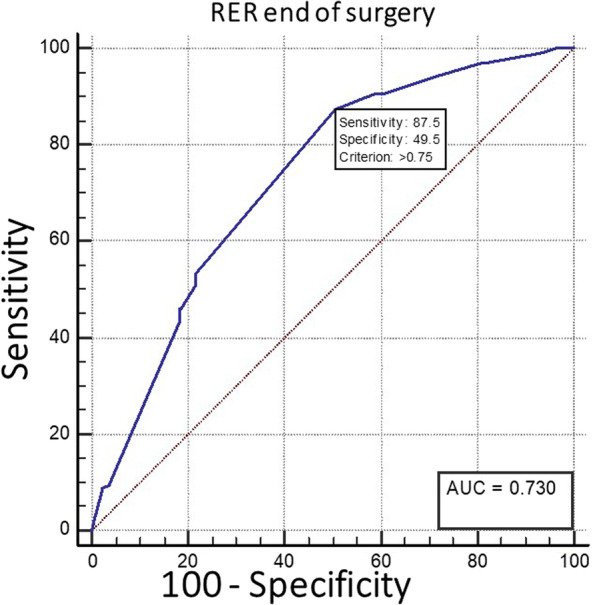
This historical cohort study included all consecutive patients who underwent intermediate-to-high risk surgery from January 1st, 2014, to April 30th, 2019 except those who did not have RER and/or arterial lactate measured. Blood lactate levels were measured routinely at the beginning and end of surgery and RER was calculated at the same moment as the blood gas sampling. The present study tested the hypothesis that RER measured at the end of surgery could detect hyperlactatemia at that time. A receiver operating characteristic (ROC) curve was constructed to assess if RER calculated at the end of the surgery could detect hyperlactatemia. The chosen RER threshold corresponded to the highest value of the sum of the specificity and the sensitivity (Youden Index).
Among the 996 patients available in our study cohort, 941 were included and analyzed. The area under the ROC curve was 0.73 (95% CI: 0.70 to 0.76; p < 0.001), with a RER threshold of 0.75, allowing to discriminate a lactate > 1.5 mmol/L with a sensitivity of 87.5% and a specificity of 49.5%.
In mechanically ventilated patients undergoing intermediate to high-risk abdominal surgery, the RER had moderate discriminative abilities to detect hyperlactatemia. Increased values should prompt clinicians to investigate for the presence of hyperlactatemia and treat any potential causes of DO/VO mismatch as suggested by the subsequent presence of hyperlactatemia.
氧输送(DO)和消耗(VO)之间不匹配与围手术期发病率和死亡率增加有关。高乳酸血症通常用作早期筛查工具,但这种非连续测量需要间歇性动脉线采样。拥有一种快速检测 DO 不足的非侵入性工具具有重要的临床意义。呼吸商(RER)可以在所有插管患者中轻松测量,并已被证明可以预测术后并发症。因此,我们旨在评估 RER 在检测接受中高危腹部手术的患者中由高乳酸血症反映的 DO 不足的能力。
本历史队列研究包括 2014 年 1 月 1 日至 2019 年 4 月 30 日期间接受中高危手术的所有连续患者,但不包括未测量 RER 和/或动脉乳酸的患者。手术开始和结束时常规测量血乳酸水平,在血气采样的同时计算 RER。本研究检验了 RER 在手术结束时测量是否可以检测到此时的高乳酸血症的假设。构建了接受者操作特征(ROC)曲线,以评估手术结束时计算的 RER 是否可以检测高乳酸血症。选择的 RER 阈值对应于特异性和敏感性(Youden 指数)之和的最高值。
在我们的研究队列中,有 996 名患者可用,其中 941 名被纳入并进行了分析。ROC 曲线下面积为 0.73(95%CI:0.70 至 0.76;p<0.001),RER 阈值为 0.75,允许以 87.5%的敏感性和 49.5%的特异性区分乳酸>1.5mmol/L。
在接受中高危腹部手术的机械通气患者中,RER 具有中等的区分能力来检测高乳酸血症。增加的值应促使临床医生调查高乳酸血症的存在,并根据随后存在的高乳酸血症治疗任何潜在的 DO/VO 不匹配的原因。