Enomoto Sayako, Yoshihara Kosuke, Kondo Eiji, Iwata Akiko, Tanaka Mamoru, Tabata Tsutomu, Kudo Yoshiki, Kondoh Eiji, Mandai Masaki, Sugiyama Takashi, Okamoto Aikou, Saito Tsuyoshi, Enomoto Takayuki, Ikeda Tomoaki
Department of Obstetrics and Gynecology, Mie University School of Medicine, Tsu 514-8507, Japan.
Department of Obstetrics and Gynecology, Niigata University Graduate School of Medical and Dental Sciences, Niigata 951-8510, Japan.
Cancers (Basel). 2022 Jun 23;14(13):3072. doi: 10.3390/cancers14133072.
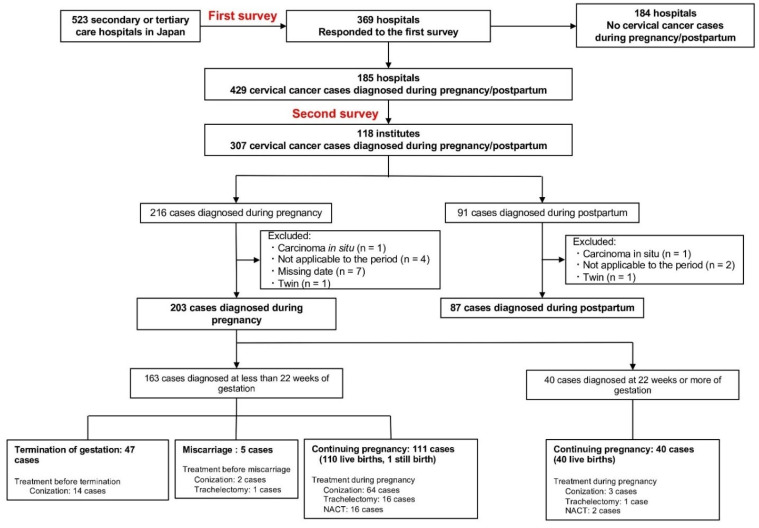
Large-scale data on maternal and neonatal outcomes of pregnancy-associated cervical cancer in Japan are scarce, and treatment strategies have not been established. This multicenter retrospective observational study investigated clinical features and trends in pregnancy-associated cervical cancer treatments at 523 hospitals in Japan. We included cervical cancer cases that were histologically diagnosed (between 1 January 2012, and 31 December 2017), and their clinical information was retrospectively collected. Of 40 patients diagnosed with pregnancy-associated cervical cancer at ≥22 gestational weeks, 34 (85.0%) were carefully followed until delivery without intervention. Of 163 diagnosed at <22 gestational weeks, 111 continued and 52 terminated their pregnancy. Ninety patients with stage IB1 disease had various treatment options, including termination of pregnancy. The 59 stage IB1 patients who continued their pregnancy were categorized by the primary treatment into strict follow-up, conization, trachelectomy, and neoadjuvant chemotherapy groups, with no significant differences in progression-free or overall survival. The birth weight percentile at delivery was smaller in the neoadjuvant chemotherapy group than in the strict follow-up group (p = 0.029). Full-term delivery rate was relatively higher in the trachelectomy group (35%) than in the other groups. Treatment decisions for pregnancy-associated cervical cancer are needed after estimating the stage, considering both maternal and fetal benefits.
日本关于妊娠相关宫颈癌孕产妇及新生儿结局的大规模数据稀缺,且尚未确立治疗策略。这项多中心回顾性观察研究调查了日本523家医院妊娠相关宫颈癌治疗的临床特征及趋势。我们纳入了经组织学诊断的宫颈癌病例(2012年1月1日至2017年12月31日期间),并回顾性收集了其临床信息。在40例诊断为妊娠相关宫颈癌且孕周≥22周的患者中,34例(85.0%)在未进行干预的情况下被密切随访至分娩。在163例诊断时孕周<22周的患者中,111例继续妊娠,52例终止妊娠。90例IB1期疾病患者有多种治疗选择,包括终止妊娠。59例继续妊娠的IB1期患者按主要治疗方法分为严格随访、锥切术、宫颈切除术及新辅助化疗组,无进展生存期或总生存期无显著差异。新辅助化疗组分娩时的出生体重百分位数低于严格随访组(p = 0.029)。宫颈切除术组的足月分娩率(35%)相对高于其他组。在评估分期后,需要综合考虑母体和胎儿的利益来做出妊娠相关宫颈癌的治疗决策。