Center for Healthcare Organization and Implementation Research, VA Boston Health Care System Jamaica Plain Campus, Boston, Massachusetts, USA
Boston University School of Public Health, Health Law, Policy & Management, Boston, Massachusetts, USA.
BMJ Open Diabetes Res Care. 2022 Jul;10(4). doi: 10.1136/bmjdrc-2021-002738.
We assessed the association between hemoglobin A1c time in range (A1c TIR), based on unique patient-level A1c target ranges, with risks of developing microvascular and macrovascular complications in older adults with diabetes.
We used a retrospective observational study design and identified patients with diabetes from the Department of Veterans Affairs (n=397 634). Patients were 65 years and older and enrolled in Medicare during the period 2004-2016. Patients were assigned to individualized A1c target ranges based on estimated life expectancy and the presence or absence of diabetes complications. We computed A1c TIR for patients with at least four A1c tests during a 3-year baseline period. The association between A1c TIR and time to incident microvascular and macrovascular complications was studied in models that included A1c mean and A1c SD.
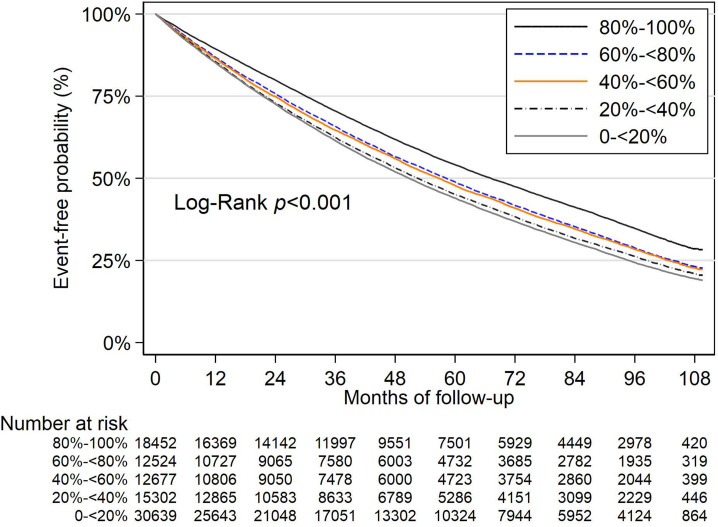
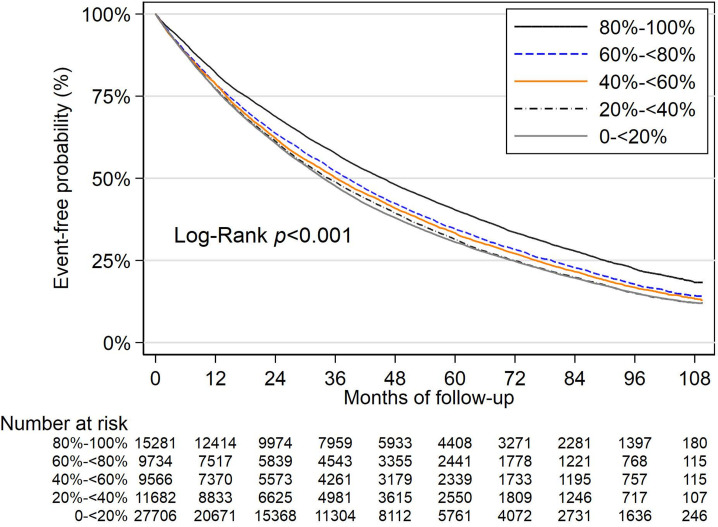
We identified 74 016 patients to assess for incident microvascular complications and 89 625 patients to assess for macrovascular complications during an average follow-up of 5.5 years. Cox proportional hazards models showed lower A1c TIR was associated with higher risk of microvascular (A1c TIR 0% to <20%; HR=1.04; 95%) and macrovascular complications (A1c TIR 0% to <20%; HR=1.07; 95%). A1c mean was associated with increased risk of microvascular and macrovascular complications but A1c SD was not. The association of A1c TIR with incidence and progression of individual diabetes complications within the microvascular and macrovascular composites showed similar trends.
Maintaining stability of A1c levels in unique target ranges was associated with lower likelihood of developing microvascular and macrovascular complications in older adults with diabetes.
我们评估了基于独特患者个体糖化血红蛋白(HbA1c)目标范围的 HbA1c 达标时间(TIR)与老年糖尿病患者微血管和大血管并发症风险之间的关系。
我们采用回顾性观察性研究设计,从退伍军人事务部(VA)中确定了糖尿病患者(n=397634)。患者年龄在 65 岁及以上,在 2004-2016 年期间参加了医疗保险。根据预期寿命和是否存在糖尿病并发症,为患者分配个体化的 HbA1c 目标范围。我们计算了至少有四次 HbA1c 检测的患者在 3 年基线期内的 HbA1c TIR。在包含 HbA1c 平均值和标准差的模型中,研究了 HbA1c TIR 与微血管和大血管并发症发生时间之间的关联。
我们确定了 74016 例患者用于评估微血管并发症的发生,89625 例患者用于评估大血管并发症的发生,平均随访时间为 5.5 年。Cox 比例风险模型显示,较低的 HbA1c TIR 与微血管(HbA1c TIR 0%至<20%;HR=1.04;95%)和大血管并发症(HbA1c TIR 0%至<20%;HR=1.07;95%)风险增加相关。HbA1c 平均值与微血管和大血管并发症风险增加相关,但 HbA1c 标准差不相关。在微血管和大血管复合体内,HbA1c TIR 与个体糖尿病并发症的发生和进展之间的关联也显示出相似的趋势。
在老年糖尿病患者中,维持独特目标范围内的 HbA1c 水平稳定与微血管和大血管并发症发生风险降低相关。