Shi Nan, Kang Jianbang, Wang Shuyun, Song Yan, Yin Donghong, Li Xiaoxia, Guo Qian, Duan Jinju, Zhang Shuqiu
Department of Pharmacy, Shanxi Medical University, Taiyuan, Shanxi, People's Republic of China.
Department of Pharmacy, Second Hospital of Shanxi Medical University, Taiyuan, Shanxi, People's Republic of China.
Infect Drug Resist. 2022 Jul 6;15:3561-3578. doi: 10.2147/IDR.S370326. eCollection 2022.
The aim of this study was to analyze the epidemiological of gram-negative bloodstream infection (GNBSI) and establish a risk prediction model for mortality and acquiring multidrug resistant (MDR), the extended spectrum beta-lactamases (ESBLs) producing and carbapenem-resistant (CR) GNBSI.
This retrospective study covered five years from January 2015 to December 2019. Data were obtained from Hospital Information System (HIS) and microbiology department records. The risk factors for mortality and acquiring MDR, ESBLs-producing and CR GNBSI were analyzed by univariable and multivariable analysis.
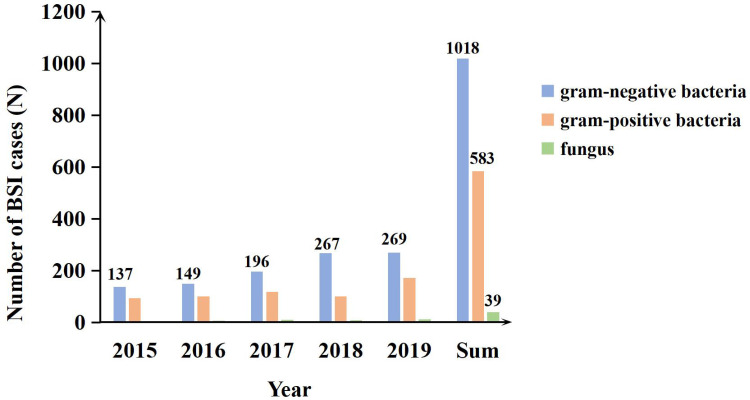
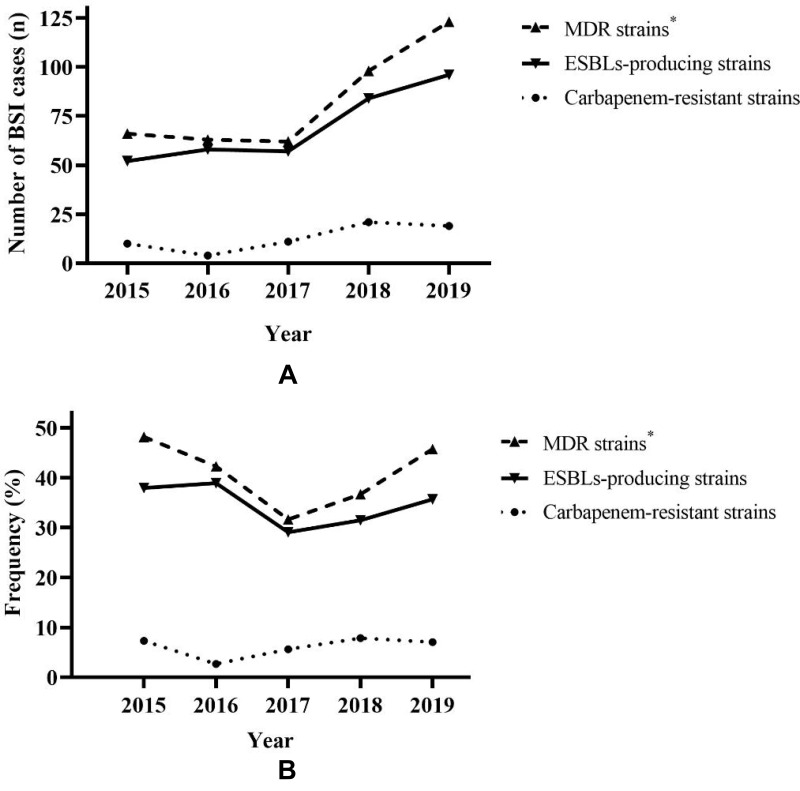
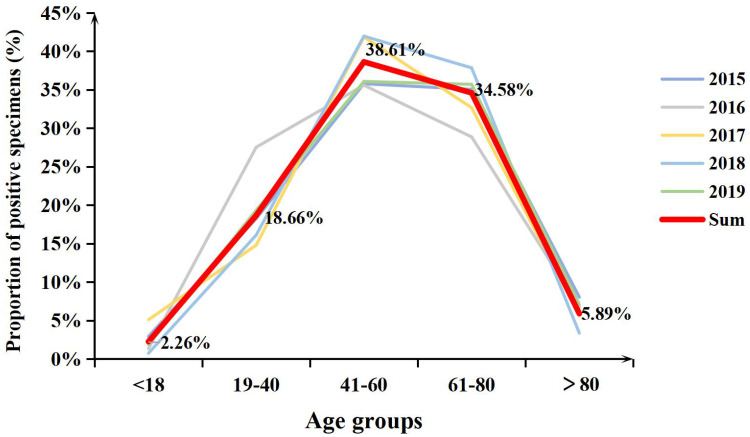
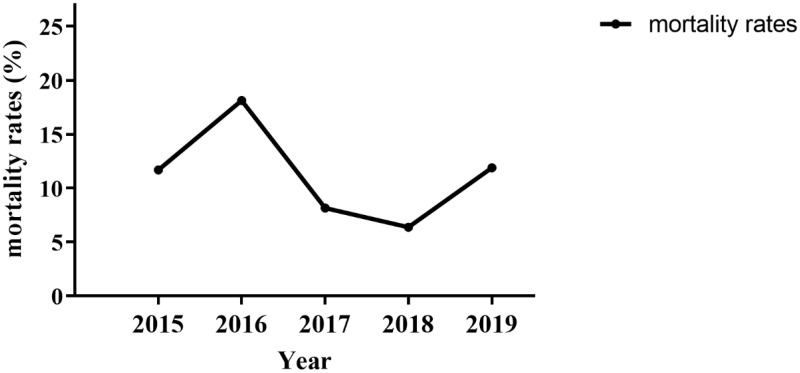
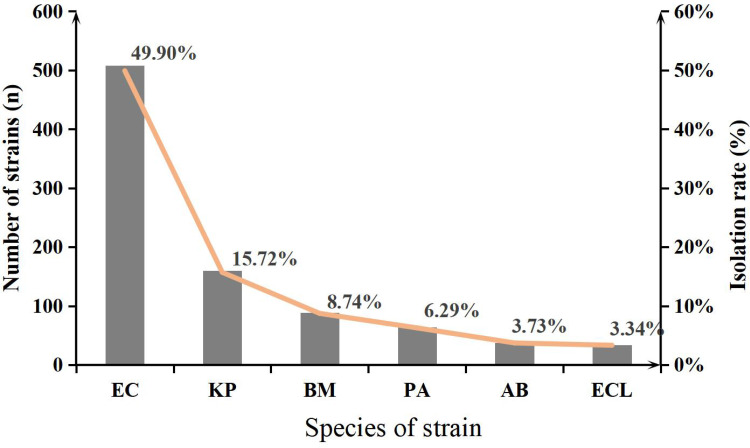
A total of 1018 GNBSI cases were collected. A majority of GNBSI patients were in hematology ward (23.77%). There were 38.61% patients who were assigned in the 41-60 age group. was the most common gram-negative organism (49.90%). Among isolates of GNBSI, 40.47% were found to be MDR strains, 34.09% were found to be ESBLs-producing strains and 7.06% were found to be CR strains. was the most common MDR (71.36%) and ESBLs-producing strain (77.81%). was the most common CR isolate (46.15%). Multivariate analysis indicated that diabetes mellitus, solid organ tumor, non-fermentative bacteria, MDR strain, central venous cannula, urinary catheter, therapy with carbapenems or tigecycline prior 30 days of infection were independent mortality risk factors for GNBSIs. Over all, therapy with tigecycline prior 30 days of infection was the mutual predictor for mortality of GNBSI, acquiring MDR, ESBLs-producing and CR GNBSI (OR, 8.221, OR, 3.963, OR, 3.588, OR, 9.222, respectively, all < 0.001).
Collectively, our study implies that patients who were diagnosed as GNBSI had a younger age. Therapy with tigecycline was the mutual and paramount predictor for mortality of GNBSI, acquiring MDR, ESBLs-producing and CR GNBSI. Our investigation had provided a theoretical basis for the use of antibiotics and prevention and control of hospital infection in our region.
本研究旨在分析革兰氏阴性菌血流感染(GNBSI)的流行病学特征,并建立死亡率以及获得多重耐药(MDR)、产超广谱β-内酰胺酶(ESBLs)和耐碳青霉烯类(CR)GNBSI的风险预测模型。
这项回顾性研究涵盖了2015年1月至2019年12月的五年时间。数据来自医院信息系统(HIS)和微生物科记录。通过单变量和多变量分析来分析死亡率以及获得MDR、产ESBLs和CR GNBSI的风险因素。
共收集到1018例GNBSI病例。大多数GNBSI患者在血液科病房(23.77%)。38.61%的患者年龄在41至60岁组。 是最常见的革兰氏阴性菌(49.90%)。在GNBSI分离株中,发现40.47%为MDR菌株,34.09%为产ESBLs菌株,7.06%为CR菌株。 是最常见的MDR(71.36%)和产ESBLs菌株(77.81%)。 是最常见的CR分离株(46.15%)。多变量分析表明,糖尿病、实体器官肿瘤、非发酵菌、MDR菌株、中心静脉导管、导尿管、感染前30天使用碳青霉烯类或替加环素治疗是GNBSIs独立的死亡风险因素。总体而言,感染前30天使用替加环素治疗是GNBSI死亡率、获得MDR、产ESBLs和CR GNBSI的共同预测因素(OR分别为8.221、3.963、3.588、9.222,均<0.001)。
总体而言,我们的研究表明,被诊断为GNBSI的患者年龄较轻。使用替加环素治疗是GNBSI死亡率、获得MDR、产ESBLs和CR GNBSI的共同且首要预测因素。我们的调查为我们地区抗生素的使用以及医院感染的防控提供了理论依据。