Kucharik Michael P, Abraham Paul F, Nazal Mark R, Varady Nathan H, Eberlin Christopher T, Meek Wendy M, Martin Scott D
Sports Medicine Center, Department of Orthopaedic Surgery, Massachusetts General Hospital, Mass General Brigham, Boston, Massachusetts, USA.
Keck School of Medicine of the University of Southern California, Los Angeles, California, USA.
Orthop J Sports Med. 2022 Jul 7;10(7):23259671221109012. doi: 10.1177/23259671221109012. eCollection 2022 Jul.
Arthroscopic treatment for labral tears includes debridement and repair. Long-term studies have failed to demonstrate a difference between these treatments in terms of conversion to total hip arthroplasty (THA).
To investigate 2 different labral treatments, debridement and repair, using an adjusted analysis to evaluate long-term conversion to THA.
Cohort study; Level of evidence, 3.
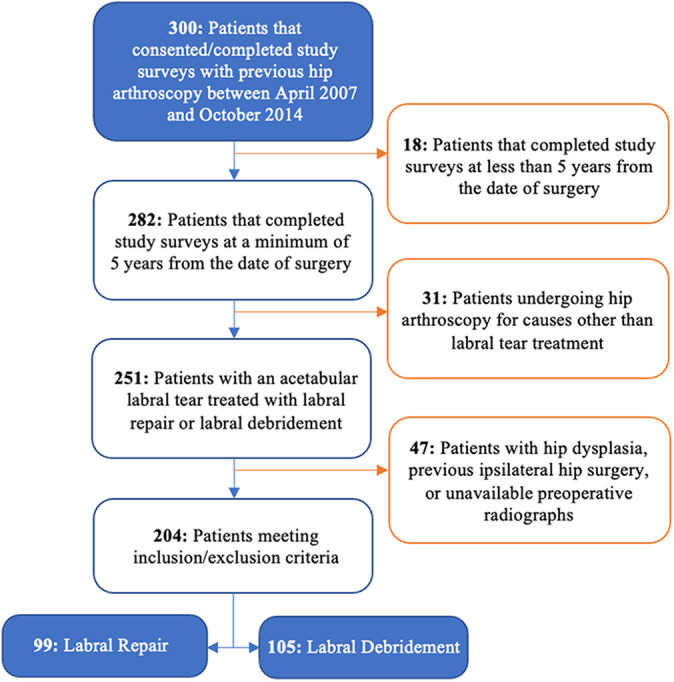
This was a retrospective cohort study of patients who underwent hip arthroscopy by a single surgeon between April 2007 and October 2014. Postoperative follow-up information included conversion to THA, patient satisfaction, and patient-reported outcome measures (modified Harris Hip Score; Hip Outcome Score, Activities of Daily Living and Sports Specific subscales; International Hip Outcome Tool; Nonarthritic Hip Score; and Lower Extremity Functional Scale).
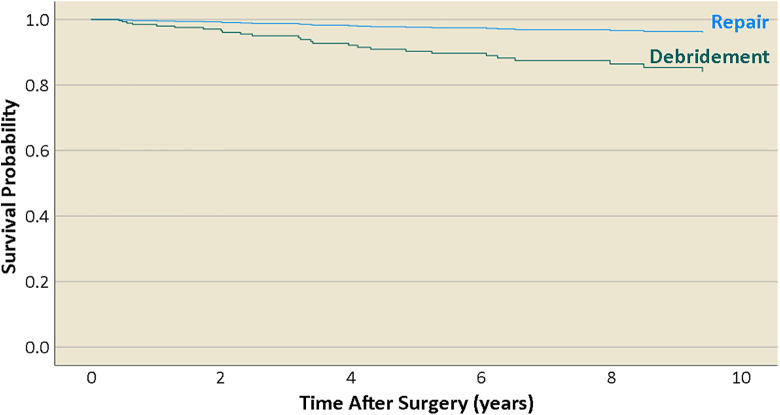
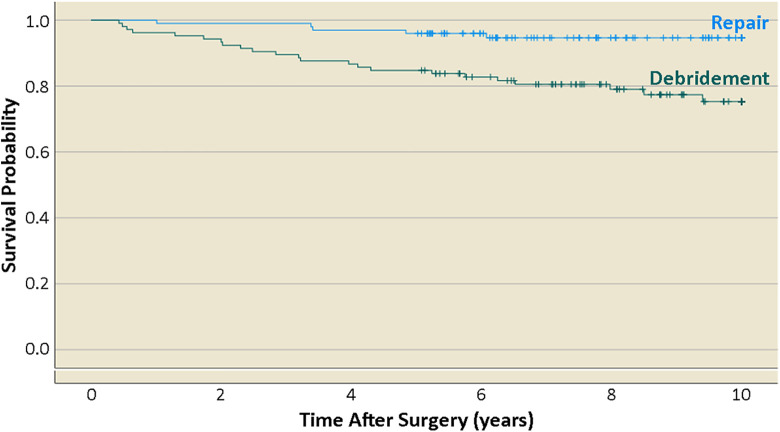
Of the 204 hips included in the study, 99 (48.5%) underwent labral repair, and 105 (51.5%) underwent debridement. In total, 28 (13.7%) of the 204 patients underwent conversion to THA within 10 years after hip arthroscopy (labral repair: 5 [5.0%] vs labral debridement: 23 [21.9%]). Labral repair was associated with a significantly lower risk of conversion to THA compared with debridement (hazard ratio [HR] = 0.24; 95% CI, 0.07-0.74; = .014). Additional factors associated with risk of conversion to THA included older age at the time of arthroscopy (HR = 1.06 per year; 95% CI, 1.02-1.11; = .002) and Tönnis grade (HR = 2.39; CI, 1.14-5.41; = .026). Abrasion chondroplasty, acetabuloplasty, body mass index, Outerbridge grade, and radiographic femoroacetabular impingement were not found to be significantly associated with risk of THA. No significant difference in patient satisfaction was found between treatment groups, and for patients who did not convert to THA, there was no difference in mean patient-reported outcome scores at final follow-up.
Patients who underwent labral repair were less likely to convert to THA compared with patients who underwent labral debridement, despite adjustment for differences in baseline patient characteristics and preexisting pathology. Additional factors associated with a lower rate of hip survival were older age and osteoarthritis at the time of hip arthroscopy.
关节镜下治疗盂唇撕裂包括清创术和修复术。长期研究未能证明这些治疗方法在全髋关节置换术(THA)转化率方面存在差异。
研究两种不同的盂唇治疗方法,即清创术和修复术,采用调整分析来评估长期THA转化率。
队列研究;证据等级,3级。
这是一项对2007年4月至2014年10月间由单一外科医生进行髋关节镜检查的患者的回顾性队列研究。术后随访信息包括THA转化率、患者满意度以及患者报告的结局指标(改良Harris髋关节评分;髋关节结局评分、日常生活活动和运动特定子量表;国际髋关节结局工具;非关节炎髋关节评分;以及下肢功能量表)。
在纳入研究的204例髋关节中,99例(48.5%)接受了盂唇修复,105例(51.5%)接受了清创术。在204例患者中,共有28例(13.7%)在髋关节镜检查后10年内接受了THA转换(盂唇修复:5例[5.0%] vs盂唇清创:23例[21.9%])。与清创术相比,盂唇修复与THA转换风险显著降低相关(风险比[HR]=0.24;95%可信区间,0.07 - 0.74;P = 0.014)。与THA转换风险相关的其他因素包括关节镜检查时年龄较大(HR = 每年1.06;95%可信区间,1.02 - 1.11;P = 0.002)和Tönnis分级(HR = 2.39;可信区间,1.14 - 5.41;P = 0.026)。未发现磨损性软骨成形术、髋臼成形术、体重指数、Outerbridge分级和影像学股骨髋臼撞击与THA风险有显著关联。治疗组之间患者满意度无显著差异,对于未转换为THA的患者,最终随访时患者报告的平均结局评分无差异。
尽管对基线患者特征和既往病理差异进行了调整,但与接受盂唇清创术的患者相比,接受盂唇修复术的患者转换为THA的可能性较小。与髋关节生存率较低相关的其他因素是髋关节镜检查时年龄较大和骨关节炎。