Department of Orthopedic Surgery, Yangpu Hospital, Tongji University School of Medicine, 450 Tengyue Road, Shanghai, 200090, People's Republic of China.
J Orthop Surg Res. 2022 Jul 15;17(1):346. doi: 10.1186/s13018-022-03236-9.
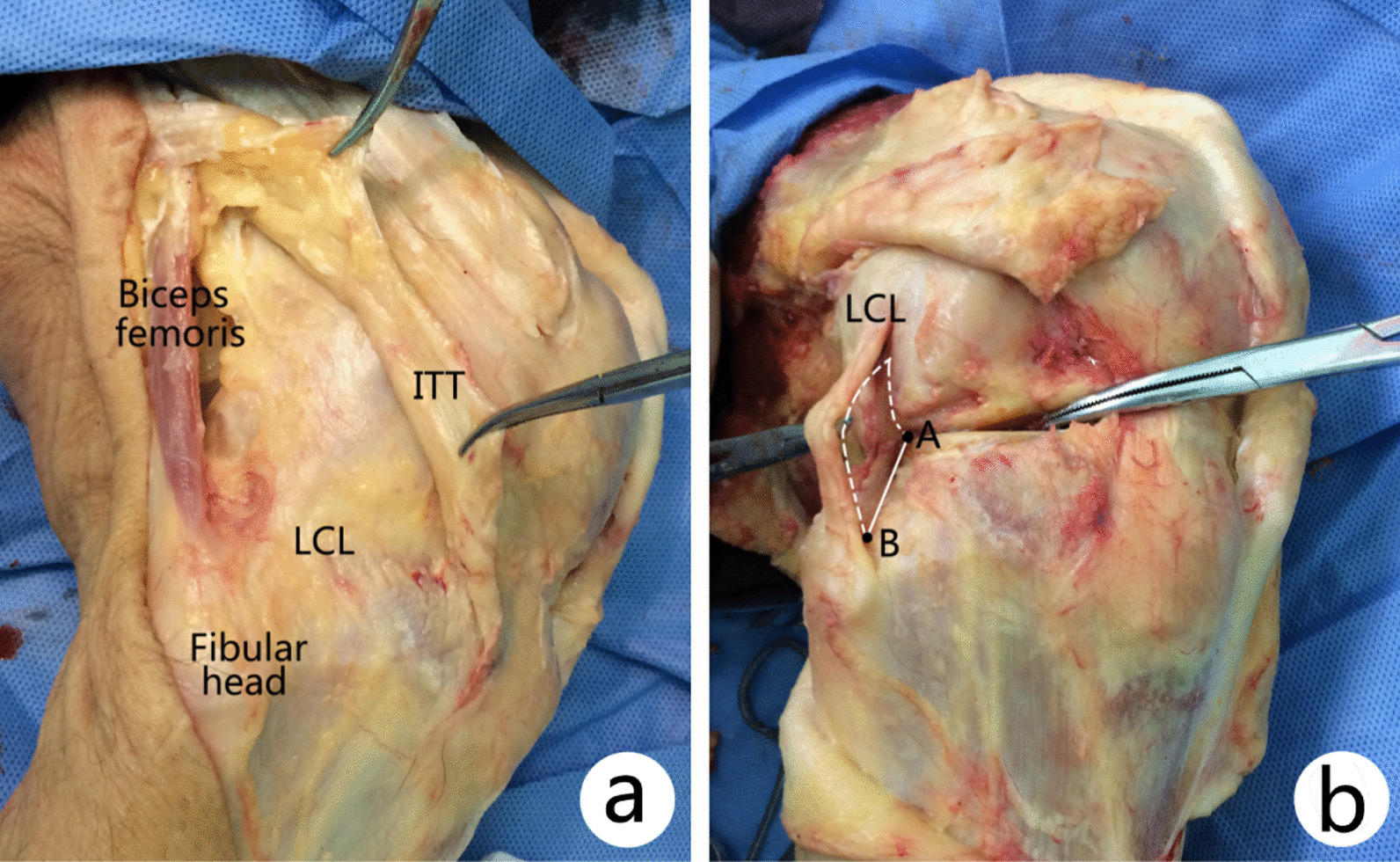
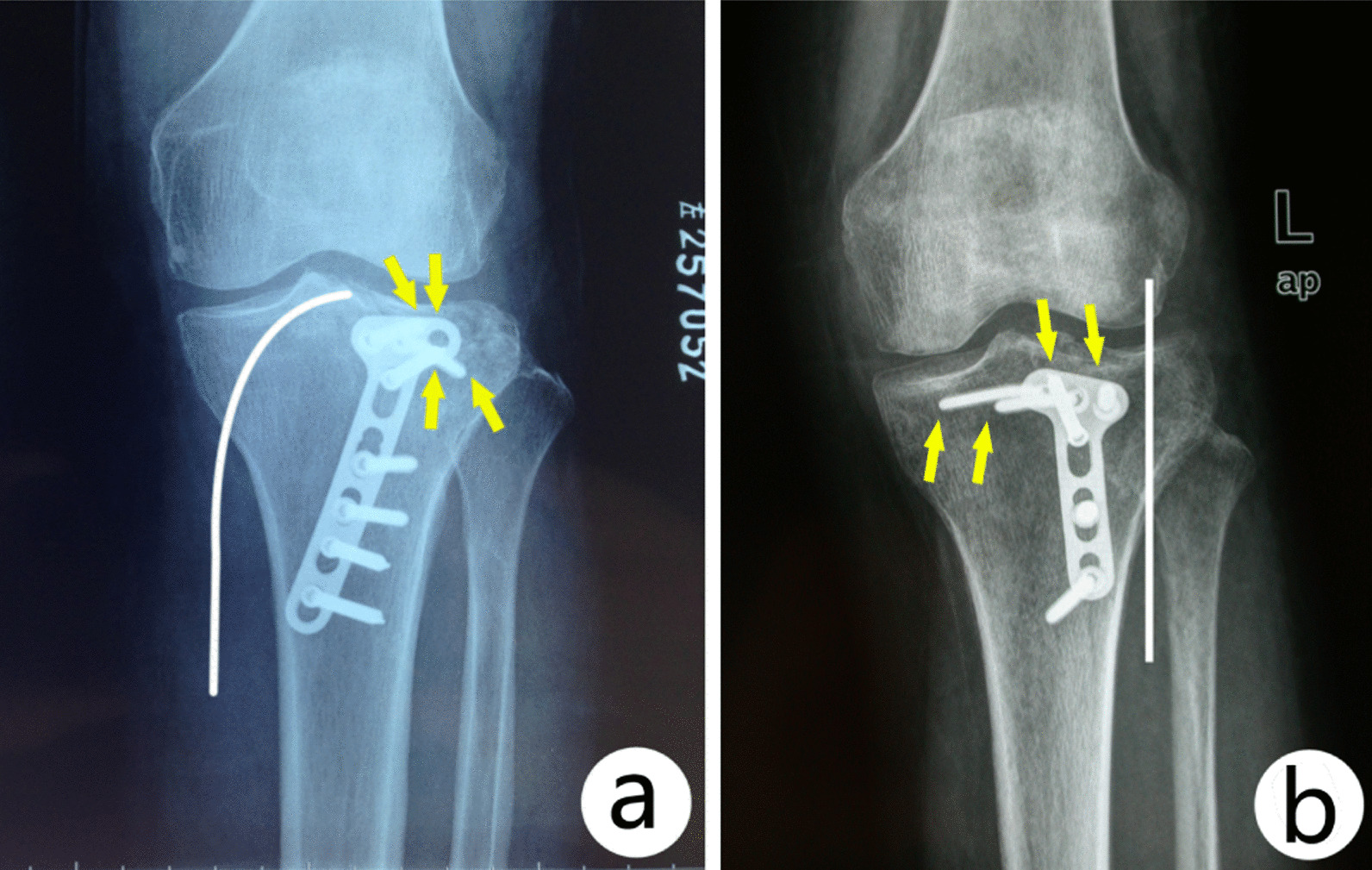
Management of posterolateral tibial plateau quadrant fractures can be challenging, and two posterior approaches were frequently used for exposure, reduction, and fixation: posterolateral approach and posteromedial approach. The purpose of this study was to compare their deep anatomical structure and analyze their limits and the risk of injury to important structures during surgical dissection of two approaches.
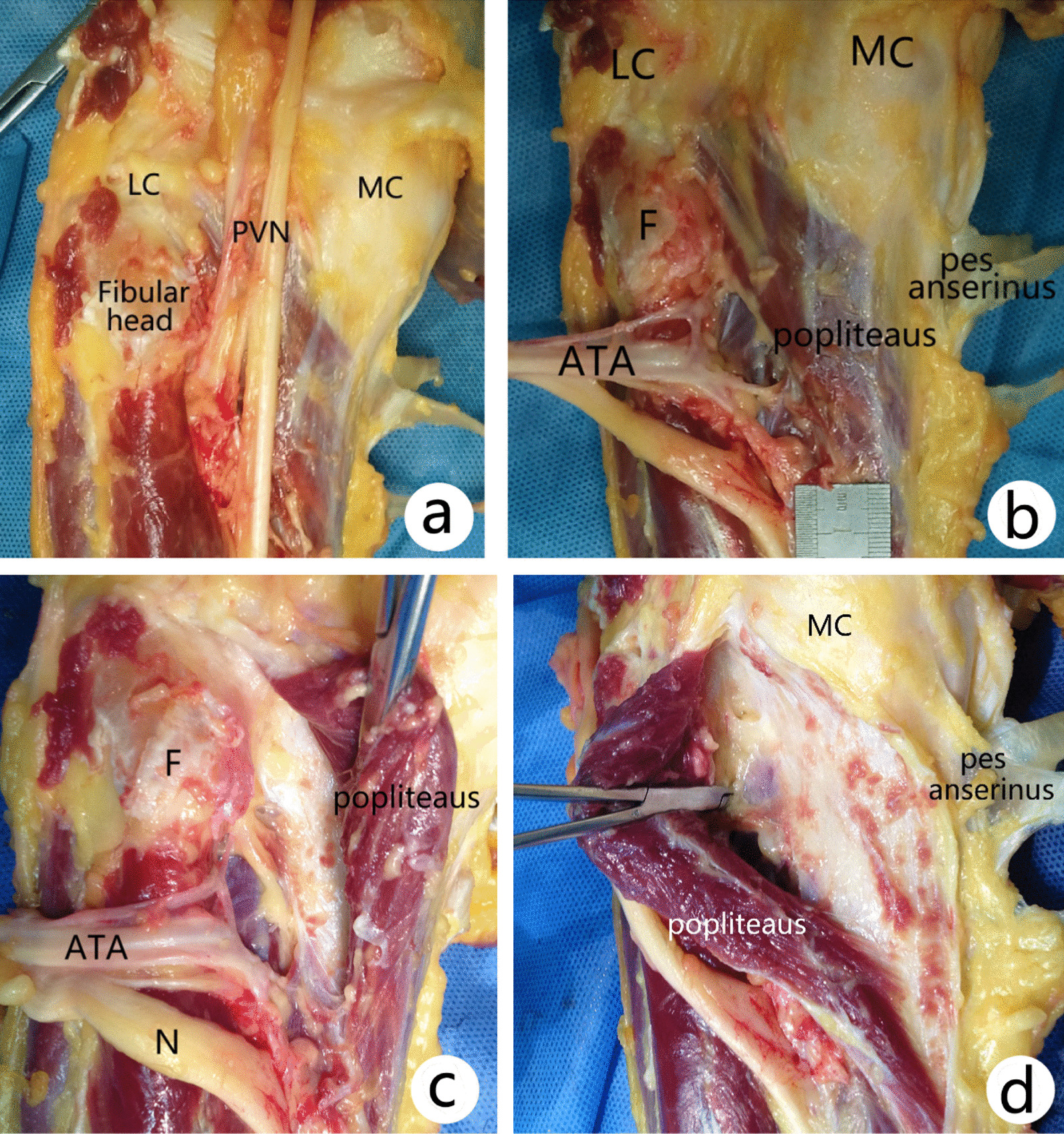
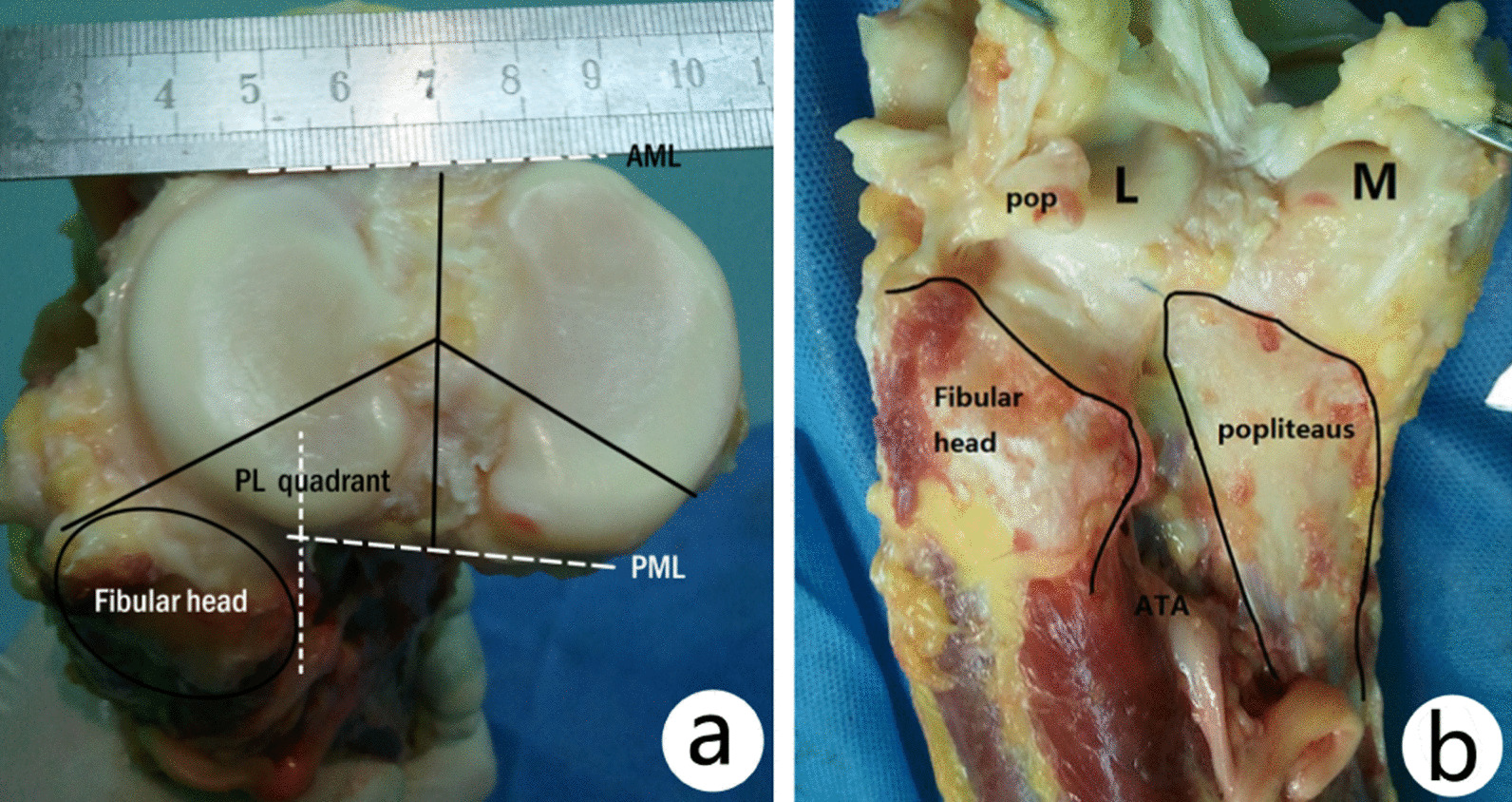
Five lower limb specimens were used in this study. After dissection of the skin and superficial fascia of each specimen, deep structures were dissected via posteromedial and posterolateral approach, and several parameters including perpendicular distance from the anterior tibial artery coursing through the interosseous membrane fissure to the lateral joint line and apex of fibular head and so on were measured and analyzed.
The perpendicular distance from the ATA coursing through the interosseous membrane fissure to the lateral joint line was 49.3 ± 5.6 mm (range 41.3-56.7 mm), while the distance to the apex of fibular head was 37.7 ± 7.2 mm (range 29.0-48.0 mm). The transverse distance of the anterior tibial vascular bundle is around 10 mm. The perpendicular distance from the top accompanying vein of the ATA bundle to lateral joint line and apex of fibular head was 44.1 ± 6.3 mm and 32.5 ± 7.6 mm, respectively. The maximum proportion of posterolateral tibial plateau shielded by the fibular head from the posterior view was 61.7 ± 4.9% (range 55.6-64.1%). The average length of popliteus muscle outside the joint was 83.1 ± 6.0 mm (range 76.5-92.2 mm), and the width in the middle was 28.1 ± 4.3 mm (range 26.6-29.1 mm).
Although posterolateral approach seems more direct for exposure of posterolateral quadrant tibial plateau fracture, it has three major disadvantages in deep dissection. Posteromedial approach through the medial board of medial head of gastrocnemius-soleus may be safer, but it was hard for direct visualization of articular surface which limits it usage for only a few cases.
后外侧胫骨平台象限骨折的治疗具有挑战性,两种后入路常用于显露、复位和固定:后外侧入路和后内侧入路。本研究的目的是比较两种入路的深部解剖结构,并分析其在手术解剖过程中的局限性和损伤重要结构的风险。
本研究使用了 5 个下肢标本。在每个标本的皮肤和浅筋膜解剖后,通过后内侧和后外侧入路进行深部结构解剖,并测量和分析了一些参数,包括穿过骨间膜裂的前胫动脉至外侧关节线和腓骨头顶点的垂直距离等。
穿过骨间膜裂的 ATA 至外侧关节线的垂直距离为 49.3±5.6mm(范围 41.3-56.7mm),而到腓骨头顶点的距离为 37.7±7.2mm(范围 29.0-48.0mm)。前胫血管束的横距约为 10mm。ATA 束顶伴静脉至外侧关节线和腓骨头顶点的垂直距离分别为 44.1±6.3mm 和 32.5±7.6mm。从后视图看,腓骨头遮盖后外侧胫骨平台的比例最大为 61.7±4.9%(范围 55.6-64.1%)。关节外的比目鱼肌平均长度为 83.1±6.0mm(范围 76.5-92.2mm),中间宽度为 28.1±4.3mm(范围 26.6-29.1mm)。
虽然后外侧入路对于后外侧胫骨平台象限骨折的显露似乎更直接,但在深部解剖中有三个主要缺点。经内侧腓肠肌-比目鱼肌头部内侧板的后内侧入路可能更安全,但由于关节面的直接可视化受到限制,仅适用于少数病例。