Frazzei Giulia, van Vollenhoven Ronald F, de Jong Brigit A, Siegelaar Sarah E, van Schaardenburg Dirkjan
Department of Rheumatology and Clinical Immunology, Amsterdam Rheumatology and Immunology Centre, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam, Netherlands.
Department of Experimental Immunology, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam, Netherlands.
Front Immunol. 2022 Jun 30;13:899372. doi: 10.3389/fimmu.2022.899372. eCollection 2022.
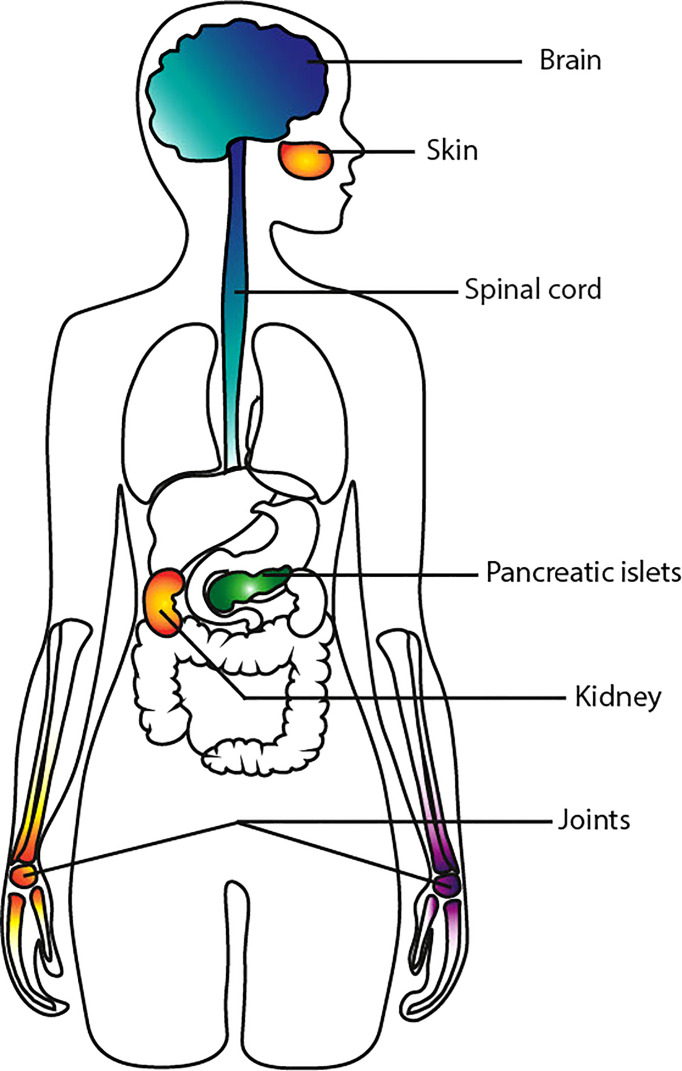
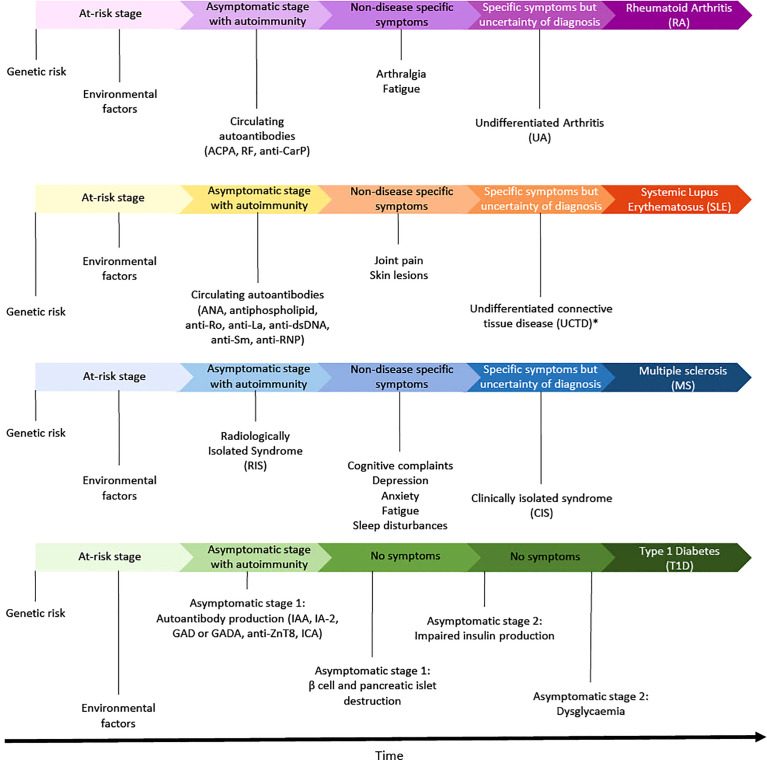
The preclinical phase of autoimmune disorders is characterized by an initial asymptomatic phase of varying length followed by nonspecific signs and symptoms. A variety of autoimmune and inflammatory manifestations can be present and tend to increase in the last months to years before a clinical diagnosis can be made. The phenotype of an autoimmune disease depends on the involved organs, the underlying genetic susceptibility and pathophysiological processes. There are different as well as shared genetic or environmental risk factors and pathophysiological mechanisms between separate diseases. To shed more light on this, in this narrative review we compare the preclinical disease course of four important autoimmune diseases with distinct phenotypes: rheumatoid arthritis (RA), Systemic Lupus Erythematosus (SLE), multiple sclerosis (MS) and type 1 diabetes (T1D). In general, we observed some notable similarities such as a North-South gradient of decreasing prevalence, a female preponderance (except for T1D), major genetic risk factors at the HLA level, partly overlapping cytokine profiles and lifestyle risk factors such as obesity, smoking and stress. The latter risk factors are known to produce a state of chronic systemic low grade inflammation. A central characteristic of all four diseases is an on average lengthy prodromal phase with no or minor symptoms which can last many years, suggesting a gradually evolving interaction between the genetic profile and the environment. Part of the abnormalities may be present in unaffected family members, and autoimmune diseases can also cluster in families. In conclusion, a promising strategy for prevention of autoimmune diseases might be to address adverse life style factors by public health measures at the population level.
自身免疫性疾病的临床前期特征为,先是一段长短不一的初始无症状期,随后出现非特异性体征和症状。可能会出现多种自身免疫性和炎症性表现,且在能够做出临床诊断的前几个月至几年中往往会增多。自身免疫性疾病的表型取决于受累器官、潜在的遗传易感性和病理生理过程。不同疾病之间存在不同但也有共同的遗传或环境风险因素以及病理生理机制。为了更清楚地了解这一点,在本篇叙述性综述中,我们比较了四种具有不同表型的重要自身免疫性疾病的临床前期病程:类风湿关节炎(RA)、系统性红斑狼疮(SLE)、多发性硬化症(MS)和1型糖尿病(T1D)。总体而言,我们观察到一些显著的相似之处,例如患病率呈南北梯度下降、女性占多数(1型糖尿病除外)、HLA水平的主要遗传风险因素、部分重叠的细胞因子谱以及肥胖、吸烟和压力等生活方式风险因素。已知后几种风险因素会导致慢性全身性低度炎症状态。所有这四种疾病的一个核心特征是,平均有一个漫长的前驱期,症状不明显或轻微,可持续多年,这表明遗传特征与环境之间的相互作用在逐渐演变。部分异常可能存在于未患病的家庭成员中,自身免疫性疾病也可能在家族中聚集。总之,预防自身免疫性疾病的一个有前景的策略可能是通过人群层面的公共卫生措施来应对不良生活方式因素。