Berthou Christian, Iliou Jean Paul, Barba Denis
Department of Immuno-Hematology INSERM UMR 12 27 LBAI University Brest Brest France.
Department of Psychiatry Pont Labbé Hospital France.
EJHaem. 2021 Dec 5;3(1):263-275. doi: 10.1002/jha2.321. eCollection 2022 Feb.
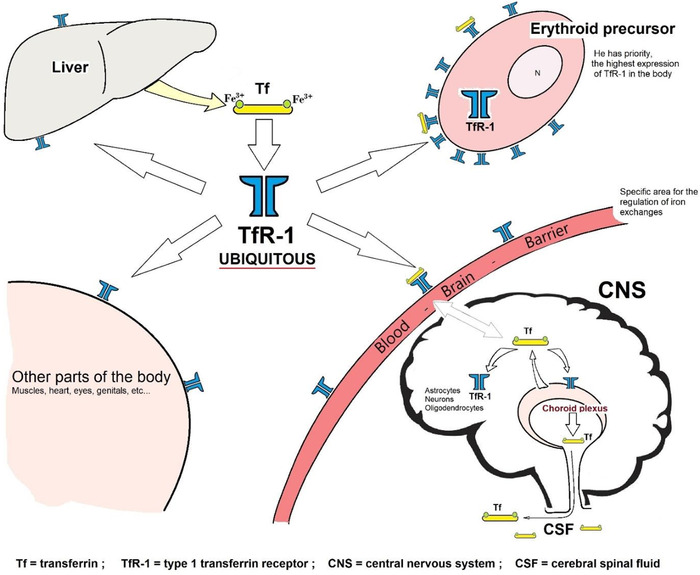
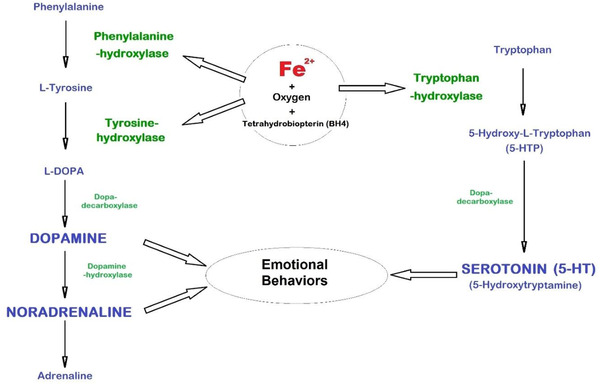
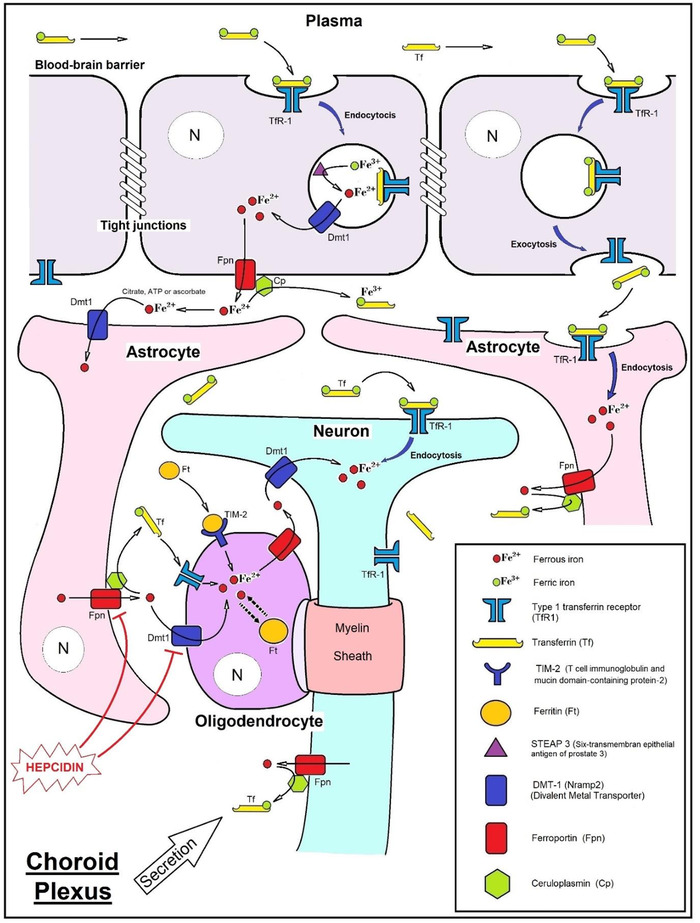
Medical management of iron deficiency (ID) requires to consider its consequences in biochemical and physiological plural functions, beyond heme/hemoglobin disrupted synthesis. Fatigue, muscle weakness, reduced exercise capacity, changes in thymia and modified emotional behaviors are the commonest symptoms integrated in the history of ID, dependent or not of the hemoglobin concentration. The relationship between depression and absolute ID (AID) is a condition which is often unrecognized. Neuro-bioavailability and brain capture of blood iron are necessary for an appropriate synthesis of neurotransmitters (serotonin, dopamine, noradrenaline). These neurotransmitters, involved in emotional behaviors, depend on neuron aromatic hydoxylases functioning with iron as essential cofactor. Noradrenaline also has impact on neuroplasticity via brain-derived neurotrophic factor (BDNF), which is key for prefrontal and hippocampus neurons playing a role in depression. Establishing the formal relationship between depression and AID remains difficult. Intracerebral reduced iron is still hard to quantify by neuroimaging and single-photon emission computed tomography (SPECT) now tends to explore the neurotransmission pathways. AID has to be looked for and identified in the context of depression, major episode or resistant to conventional treatment such as serotonin reuptake inhibitor, and even in the absence of anemia, microcytosis or hypochromia (non-anemic ID). Confronted to brain imaging, blood iron status evaluation is indicated, especially in depressed, treatment-resistant, iron-deficient young women. In patients suffering from depression, increase in the prevalence of AID should be considered, in order to deliver a suitable treatment, considering both anti-depressive program and iron supplementation if AID.
缺铁(ID)的医学管理需要考虑其在生化和生理多种功能方面的后果,而不仅仅是血红素/血红蛋白合成受阻。疲劳、肌肉无力、运动能力下降、胸腺变化和情绪行为改变是缺铁病史中最常见的症状,与血红蛋白浓度无关或有关。抑郁症与绝对缺铁(AID)之间的关系是一种常未被认识的情况。神经生物利用度和脑对血中铁的摄取对于神经递质(血清素、多巴胺、去甲肾上腺素)的适当合成是必要的。这些参与情绪行为的神经递质依赖于以铁作为必需辅因子发挥作用的神经元芳香羟化酶。去甲肾上腺素还通过脑源性神经营养因子(BDNF)对神经可塑性产生影响,BDNF对在抑郁症中起作用的前额叶和海马神经元至关重要。确立抑郁症与AID之间的正式关系仍然困难。脑内铁减少仍难以通过神经成像进行量化,单光子发射计算机断层扫描(SPECT)现在倾向于探索神经传递途径。在抑郁症、重度发作或对常规治疗(如血清素再摄取抑制剂)耐药的情况下,甚至在没有贫血、小红细胞症或低色素血症(非贫血性ID)的情况下,都必须寻找并识别AID。面对脑部成像时,需要评估血中铁状态,特别是在抑郁、治疗耐药、缺铁的年轻女性中。对于患有抑郁症的患者,应考虑AID患病率的增加,以便提供合适的治疗,既要考虑抗抑郁方案,又要在存在AID时考虑补充铁剂。