Amasya Üniversitesi Sabuncuoğlu Şerefeddin Eğitim ve Araştırma Hastanesi, Ortopedi ve Travmatoloji Kliniği, 05200 Amasya, Türkiye.
Jt Dis Relat Surg. 2022;33(2):440-448. doi: 10.52312/jdrs.2022.526. Epub 2022 Jul 6.
The aim of this study was to identify the demographic characteristics of chondrosarcoma (CS) and prognostic factors affecting survival.
A total of 87 patients (45 males, 42 females; median age: 51.3 years; range, 19 to 77 years) with CS treated in our clinic between January 2007 and June 2020 were retrospectively analyzed. Demographic characteristics, whether it was primary/secondary, tumor location, histopathological features, tumor grade and stage, clinical follow-up period, surgical treatment methods, use of radiotherapy and chemotherapy, and the presence of local recurrence and metastasis in the postoperative period were recorded. The relationship of these factors with prognosis was analyzed and survival rates were compared.
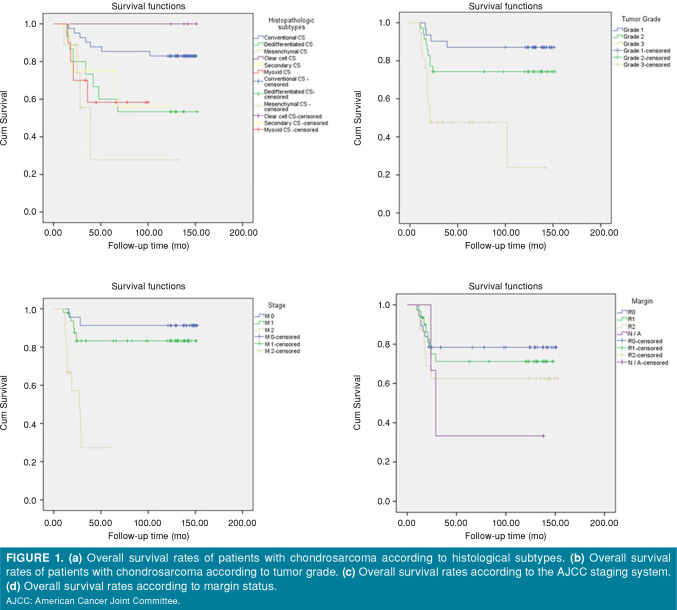
Histological subtype, tumor grade, pathological stage and presence of metastasis were defined as independent predictors in both overall survival and disease-free survival analysis of CS. Overall and disease-free five-year and 10-year survival rates were found to be the highest in the clear cell chondrosarcoma group. While mortality increased in the first five years in the patient groups with histological Grade 2 and 3, all groups were followed in a balanced manner over time. The mortality rate in the group with metastatic disease (M2) was approximately four times higher than the other groups at 10-year follow-up. According to the surgical margins, we found that the five-year survival rates of the R1 (marginal resection) and R2 (residual tumor) groups were similar, with the highest rate being in the R0 (wide resection) group with 78.3%. In multivariate analysis, only grade and stage had a significant association with disease-specific survival. Surgical resection combined with adjuvant radiotherapy was found to increase survival in both overall and disease-free survival of patients with dedifferentiated chondrosarcoma compared to other treatments.
Histological subtype, grade, stage and presence of metastasis were the independent prognostic factors for survival in CS. However, marginal resection was a risk factor for local recurrence (LR), but there was no significant difference in overall survival in patients with or without LR. Although it is not significant, radiotherapy could increase survival in dedifferentiated CS variants.
本研究旨在确定软骨肉瘤(CS)的人口统计学特征和影响生存的预后因素。
回顾性分析 2007 年 1 月至 2020 年 6 月在我院治疗的 87 例 CS 患者(男 45 例,女 42 例;中位年龄:51.3 岁;范围 19-77 岁)的临床资料。记录患者的人口统计学特征、是否为原发性/继发性、肿瘤部位、组织病理学特征、肿瘤分级和分期、临床随访期、手术治疗方法、放疗和化疗的使用情况以及术后局部复发和转移情况。分析这些因素与预后的关系,并比较生存率。
组织学亚型、肿瘤分级、病理分期和转移存在被定义为 CS 总生存和无病生存分析的独立预测因素。在透明细胞软骨肉瘤组中,总生存和无病生存 5 年和 10 年生存率最高。而在组织学分级 2 级和 3 级的患者中,前 5 年死亡率增加,但随着时间的推移,所有组的死亡率都保持平衡。在转移性疾病(M2)组中,10 年随访时的死亡率约为其他组的 4 倍。根据手术切缘,我们发现 R1(边缘切除)和 R2(残留肿瘤)组的 5 年生存率相似,而 R0(广泛切除)组的生存率最高,为 78.3%。多因素分析显示,只有分级和分期与疾病特异性生存显著相关。与其他治疗方法相比,手术切除联合辅助放疗可提高去分化软骨肉瘤患者的总生存和无病生存。
组织学亚型、分级、分期和转移是 CS 生存的独立预后因素。然而,边缘切除是局部复发(LR)的危险因素,但 LR 患者的总生存无显著差异。尽管没有显著差异,但放疗可能会增加去分化 CS 变异型的生存。