van Praag Veroniek M, Molenaar Dominique, Tendijck Guus A H, Schaap Gerard R, Jutte Paul C, van der Geest Ingrid C M, Fiocco Marta, van de Sande Michiel A J
Department of Orthopedic Surgery, Leiden University Medical Center, Albinusdreef 2, 2333 ZA Leiden, The Netherlands.
Department of Orthopedic Surgery, Amsterdam University Medical Center, Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands.
Cancers (Basel). 2024 Oct 14;16(20):3484. doi: 10.3390/cancers16203484.
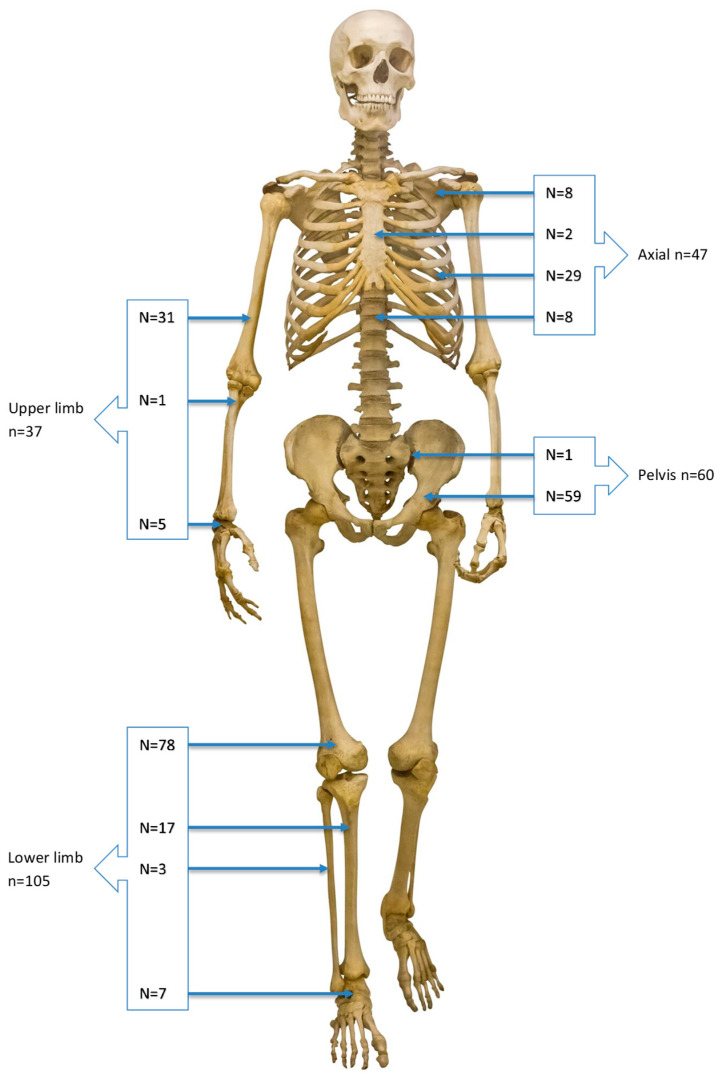
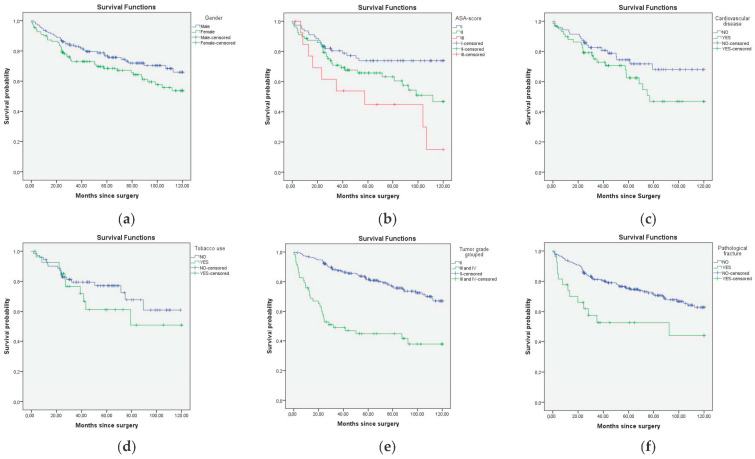
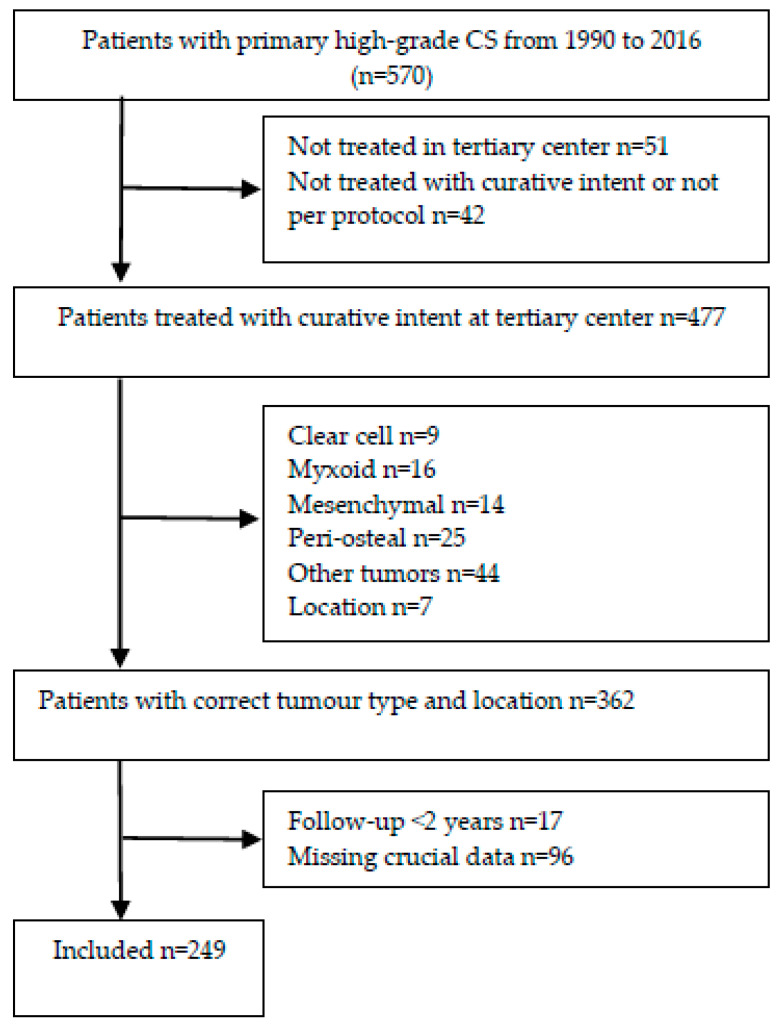
Due to the relatively advanced age and high mortality rate of patients with high-grade chondrosarcoma (CS), it is important to holistically assess patient- and tumor characteristics in multidisciplinary team and shared decision-making with regard to treatment options. While current prognostic models include multiple tumor and treatment characteristics, the only patient characteristics that are commonly included are age and gender. Based on clinical experience, we believe that factors related to patient preoperative systemic health status such as the American Society of Anesthesiologists (ASA) score may be equally important prognostic factors for overall survival (OS). A retrospective nationwide cohort study was identified from four specialized bone sarcoma centers in The Netherlands. Patients with a primary CS grade II, III, and dedifferentiated CS were eligible. Prognostic factors including age at presentation, gender, ASA score, CVD, tobacco use, BMI, histological tumor grade, tumor size, pathological fracture, presentation after unplanned excision, type of surgery and surgical margin were evaluated. The outcome measure was OS at the time of surgery. The Kaplan-Meier methodology was employed to estimate OS; a log-rank test was used to assess the difference in survival. To study the impact of prognostic factors on OS, a multivariate Cox proportional hazard regression model was estimated. In total, 249 patients were eligible for this study, and 89 were deceased at the end of follow-up. In multivariate analysis, histological grade (HR 2.247, 95% CI 1.334-3.783), ASA score III (HR 2.615, 95% CI 1.145-5.976, vs. ASA I), and age per year (HR: 1.025, 95% CI 1.004-1.045) were negatively associated with OS. No association was found between tobacco use, BMI, gender or cardiovascular disease and OS in this cohort. Pathological fracture and tumor size were only associated with OS in univariate analysis. This multicenter study is the first on sarcomas to include ASA in a prognostic model. Results show that ASA score as a proxy for patients' systemic health status should be included when providing a prognosis for patients with a high-grade primary CS, besides the conventional risk factors such as tumor grade and age. Specifically, severe systemic disease (ASA score III) is a strong negative predictor. Conversely, we found no difference in OS between ASA scores I and II. These findings aid multidisciplinary team and shared decision-making with regard to these complex sarcoma patients that often require life-changing surgeries. Prognostic level III. See the instructions for authors for the complete description of levels of evidence.
由于高级别软骨肉瘤(CS)患者年龄相对较大且死亡率较高,在多学科团队中全面评估患者特征和肿瘤特征,并就治疗方案进行共同决策非常重要。虽然目前的预后模型包括多种肿瘤和治疗特征,但通常纳入的唯一患者特征是年龄和性别。根据临床经验,我们认为与患者术前全身健康状况相关的因素,如美国麻醉医师协会(ASA)评分,可能是总生存期(OS)同样重要的预后因素。一项回顾性全国队列研究来自荷兰的四个专业骨肉瘤中心。原发性CS II级、III级和去分化CS患者符合条件。评估了预后因素,包括就诊时年龄、性别、ASA评分、心血管疾病、吸烟情况、体重指数、组织学肿瘤分级、肿瘤大小、病理性骨折、计划外切除后就诊、手术类型和手术切缘。结局指标是手术时的OS。采用Kaplan-Meier方法估计OS;使用对数秩检验评估生存差异。为了研究预后因素对OS的影响,估计了多变量Cox比例风险回归模型。总共249例患者符合本研究条件,89例在随访结束时死亡。在多变量分析中,组织学分级(HR 2.247,95%CI 1.334 - 3.783)、ASA评分III(HR 2.615,95%CI 1.145 - 5.976,与ASA I相比)和每年年龄(HR:1.025,95%CI 1.004 - 1.045)与OS呈负相关。在该队列中,未发现吸烟、体重指数、性别或心血管疾病与OS之间存在关联。病理性骨折和肿瘤大小仅在单变量分析中与OS相关。这项多中心研究是肉瘤领域首次将ASA纳入预后模型的研究。结果表明,在为高级别原发性CS患者提供预后时,除了肿瘤分级和年龄等传统风险因素外,应将ASA评分作为患者全身健康状况的指标纳入。具体而言,严重全身疾病(ASA评分III)是一个强有力的负性预测因素。相反,我们发现ASA评分I和II之间的OS没有差异。这些发现有助于多学科团队针对这些通常需要改变生活的手术的复杂肉瘤患者进行共同决策。预后水平III。有关证据水平的完整描述,请参阅作者指南。