Department of Neurology, The University of Iowa Hospitals and Clinics, Iowa City, Iowa, USA.
Institute for Clinical and Translational Science, The University of Iowa, Iowa City, Iowa, USA.
J Neurointerv Surg. 2023 Aug;15(8):747-752. doi: 10.1136/jnis-2022-019125. Epub 2022 Jul 19.
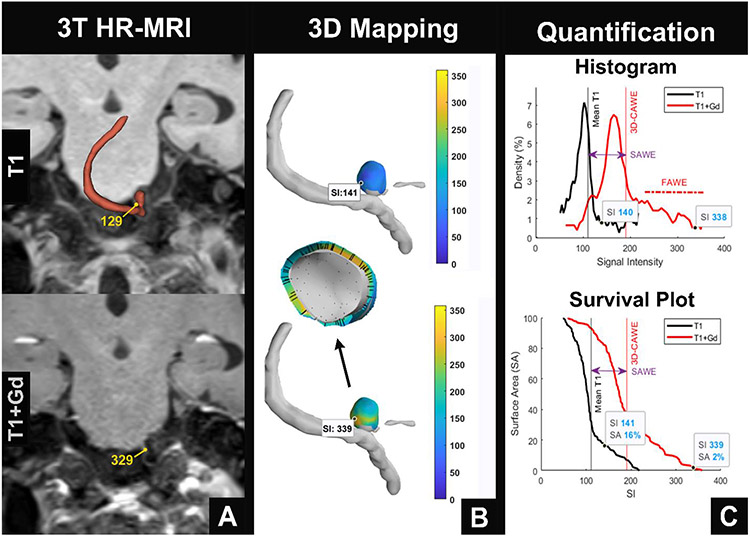
Aneurysm wall enhancement (AWE) is a potential surrogate biomarker for aneurysm instability. Previous studies have assessed AWE using 2D multiplanar methods, most of which were conducted qualitatively.
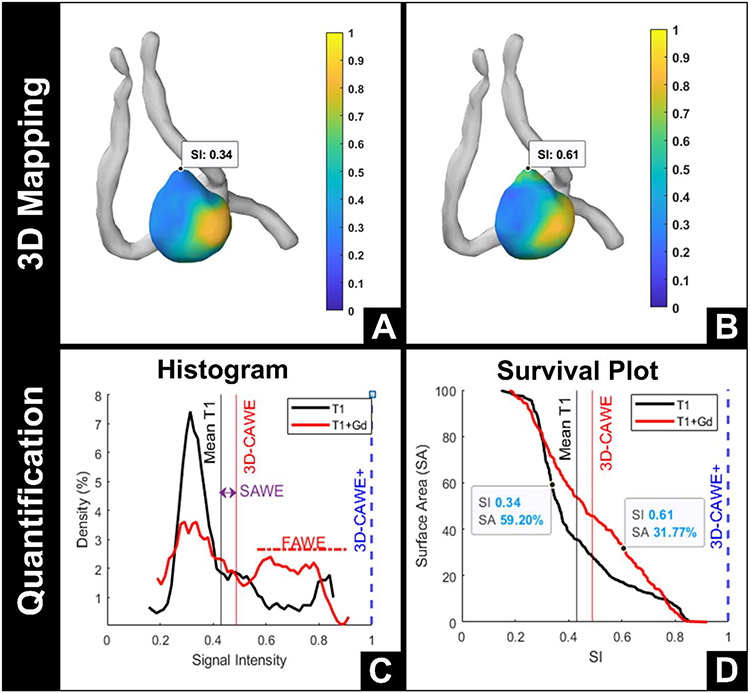
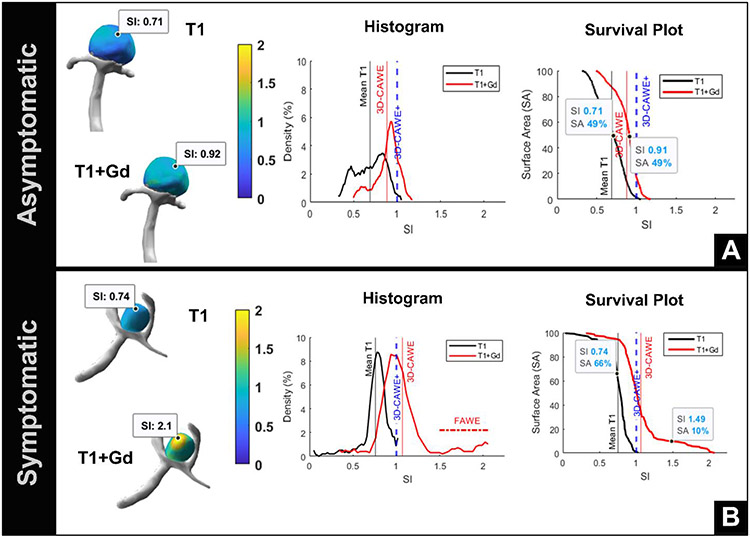
To use a new quantitative tool to analyze a large cohort of saccular aneurysms with 3D-AWE maps METHODS: Saccular aneurysms were imaged prospectively with 3T high resolution MRI. 3D-AWE maps of symptomatic (defined as ruptured or presentation with sentinel headache/cranial nerve neuropathy) and asymptomatic aneurysms were created by extending orthogonal probes from the aneurysm lumen into the wall. Three metrics were used to characterize enhancement: 3D circumferential AWE (3D-CAWE), aneurysm-specific contrast uptake (SAWE), and focal AWE (FAWE). Aneurysms with a circumferential AWE higher than the corpus callosum (3D-CAWE ≥1) were classified as 3D-CAWE+. Symptomatic presentation was analyzed with univariate and multivariate logistic models. Aneurysm size, size ratio, aspect ratio, irregular morphology, and PHASES and ELAPSS scores were compared with the new AWE metrics. Bleb and microhemorrhage analyses were also performed.
Ninety-three aneurysms were analyzed. 3D-CAWE, SAWE, and FAWE were associated with symptomatic status (OR=1.34, 1.25, and 1.08, respectively). A multivariate model including aneurysm size, 3D-CAWE+, age, female gender, and FAWE detected symptomatic status with 80% specificity and 90% sensitivity (area under the curve=0.914, =0.967). FAWE was also associated with irregular morphology and high-risk location (p=0.043 and p=0.001, respectively). In general, blebs enhanced 56% more than the aneurysm body. Areas of microhemorrhage co-localized with areas of increased SAWE (p=0.047).
3D-AWE mapping provides a new set of metrics that could potentially improve the identification of symptomatic aneurysms.
动脉瘤壁增强(AWE)是动脉瘤不稳定的潜在替代生物标志物。先前的研究使用二维多平面方法评估了 AWE,其中大多数方法都是定性的。
使用新的定量工具分析大量囊状动脉瘤的 3D-AWE 图谱。
使用 3T 高分辨率 MRI 前瞻性地对囊状动脉瘤进行成像。通过从动脉瘤管腔向壁延伸正交探针,创建有症状(定义为破裂或出现先兆性头痛/颅神经神经病)和无症状动脉瘤的 3D-AWE 图谱。使用三个指标来描述增强:三维周向 AWE(3D-CAWE)、动脉瘤特异性对比摄取(SAWE)和局灶性 AWE(FAWE)。将周向 AWE 高于胼胝体(3D-CAWE≥1)的动脉瘤归类为 3D-CAWE+。使用单变量和多变量逻辑模型分析症状表现。比较了动脉瘤大小、大小比、纵横比、不规则形态以及 PHASES 和 ELAPSS 评分与新的 AWE 指标。还进行了微泡和微出血分析。
分析了 93 个动脉瘤。3D-CAWE、SAWE 和 FAWE 与症状状态相关(OR=1.34、1.25 和 1.08)。包括动脉瘤大小、3D-CAWE+、年龄、女性性别和 FAWE 的多变量模型检测到症状状态的特异性为 80%,敏感性为 90%(曲线下面积=0.914,=0.967)。FAWE 还与不规则形态和高风险位置相关(p=0.043 和 p=0.001)。一般来说,微泡比动脉瘤体增强 56%。微出血区域与 SAWE 增加区域共定位(p=0.047)。
3D-AWE 图谱提供了一组新的指标,可能有助于提高对有症状动脉瘤的识别。