Hernández-Fernández Francisco, Cámara-González Noemí, Pedrosa-Jiménez María José, Alcahut-Rodríguez Cristian
Departments of Neurology and.
Radiology, Complejo Hospitalario Universitario de Albacete, Albacete, Spain; and.
J Neurosurg Case Lessons. 2021 May 17;1(20):CASE21123. doi: 10.3171/CASE21123.
Spontaneous spinal subdural hematomas (SSDHs) are unusual. Among their probable etiologies, an association with ruptured brain aneurysms has been described in an extraordinary way. The underlying pathophysiological mechanism is not conclusively described in the literature.
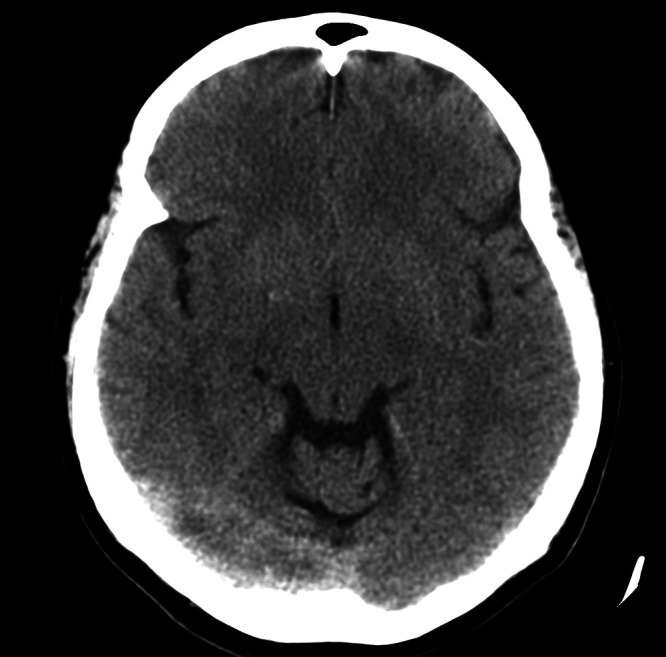
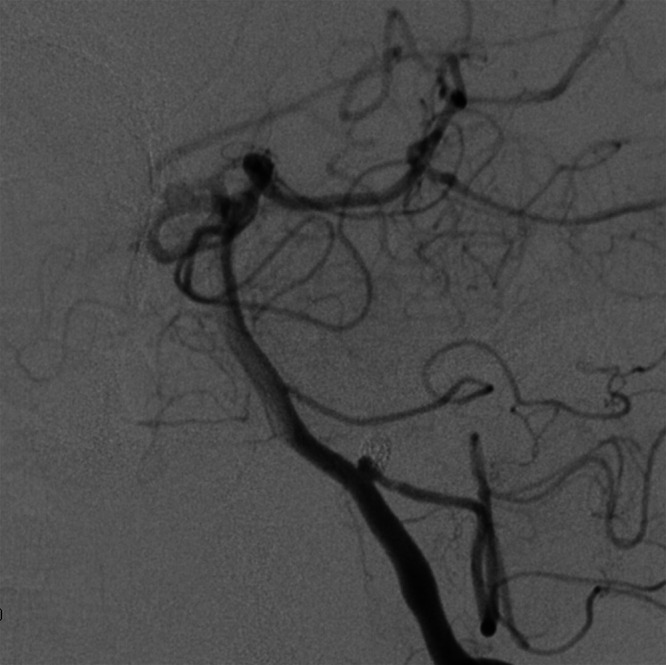
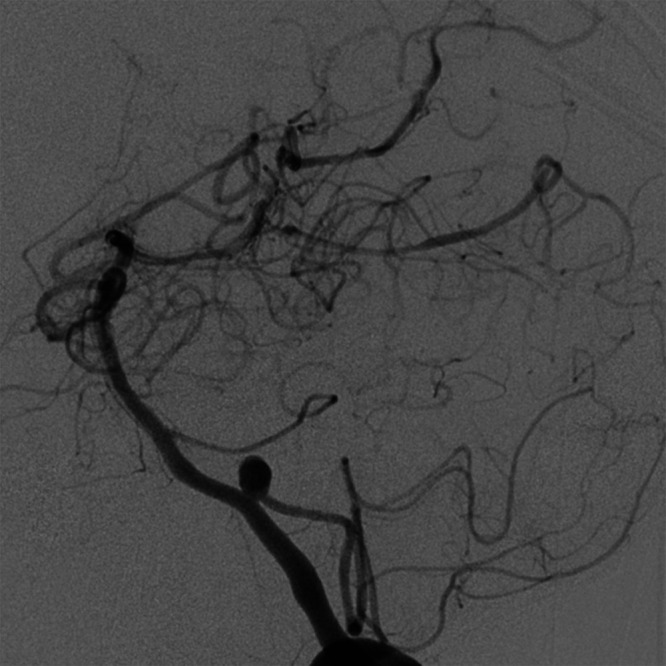
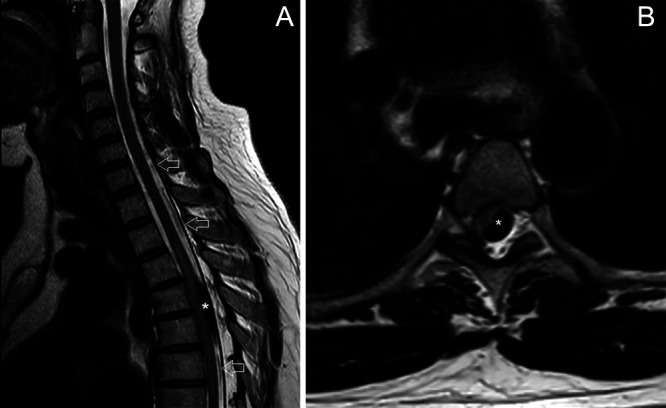
The authors reported an exceptional case of a 59-year-old woman admitted for a condition that included sudden headache, stiff neck, and vomiting associated with pain in the left flank area that radiated to the leg. Computed tomography (CT) of the brain evidenced acute subarachnoid hemorrhage distributed in the bilateral posterior parieto-occipital fossa and occipital horns of the ventricles. CT angiography detected a dissecting aneurysm in the left vertebral artery (V4) that was treated urgently via the endovascular route. In the next hours, the patient's symptoms worsened, with paraplegia of the lower extremities. Magnetic resonance imaging showed SSDH at T4-6 and extensive associated myelopathy.
The origin of the spinal hematoma may be the rupture of the aneurysm of the V4 segment in the dura mater of the foramen magnum and subsequent rostrocaudal migration of the hemorrhage to the spinal subdural space, enhanced by an intracranial pressure increase. This hypothesis is discussed, as is a brief literature review.
自发性脊髓硬膜下血肿(SSDHs)较为罕见。在其可能的病因中,与脑动脉瘤破裂的关联已有特殊描述。文献中尚未对其潜在的病理生理机制进行确切阐述。
作者报告了一例特殊病例,一名59岁女性因突发头痛、颈部僵硬、呕吐伴左侧胁腹疼痛并放射至腿部入院。脑部计算机断层扫描(CT)显示急性蛛网膜下腔出血分布于双侧后顶枕叶窝及脑室枕角。CT血管造影检测到左侧椎动脉(V4)夹层动脉瘤,遂通过血管内途径进行紧急治疗。在接下来的数小时内,患者症状恶化,出现双下肢截瘫。磁共振成像显示T4 - 6水平存在脊髓硬膜下血肿及广泛相关脊髓病。
脊髓血肿的起源可能是枕骨大孔硬膜内V4段动脉瘤破裂,随后出血因颅内压升高而向头尾方向迁移至脊髓硬膜下间隙。本文对此假说进行了讨论,并简要回顾了相关文献。