Department of Obstetrics and Gynaecology and Unit for Gynaecological Oncology, Tygerberg Hospital, Stellenbosch University, Cape Town, South Africa.
PLoS One. 2022 Jul 21;17(7):e0271526. doi: 10.1371/journal.pone.0271526. eCollection 2022.
This study aimed to determine 5-year progression-free and overall survival in patients with uterine carcinosarcoma, to determine clinical and surgical-pathologic features, to recognize patterns of recurrence and to identify prognostic factors influencing progression-free survival (PFS) and overall survival (OS).
This was a single institution, retrospective 10-year review of patients treated at Tygerberg Hospital in South Africa with pathologically confirmed uterine carcinosarcoma.
A total of 61 patients were studied. Demographic, clinicopathological, treatment and outcome information were obtained. Kaplan-Meier survival analysis and Cox proportional hazards models were used to determine the effects of variables on PFS and OS.
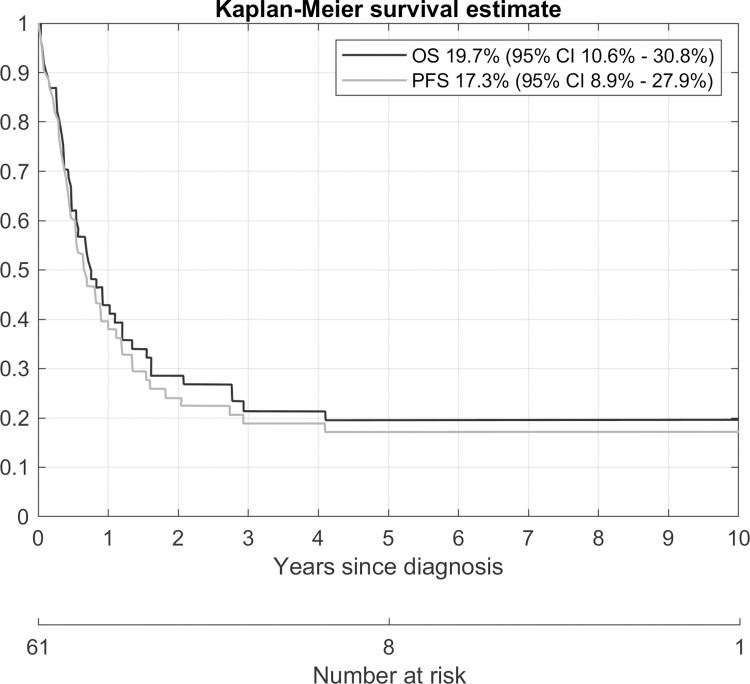
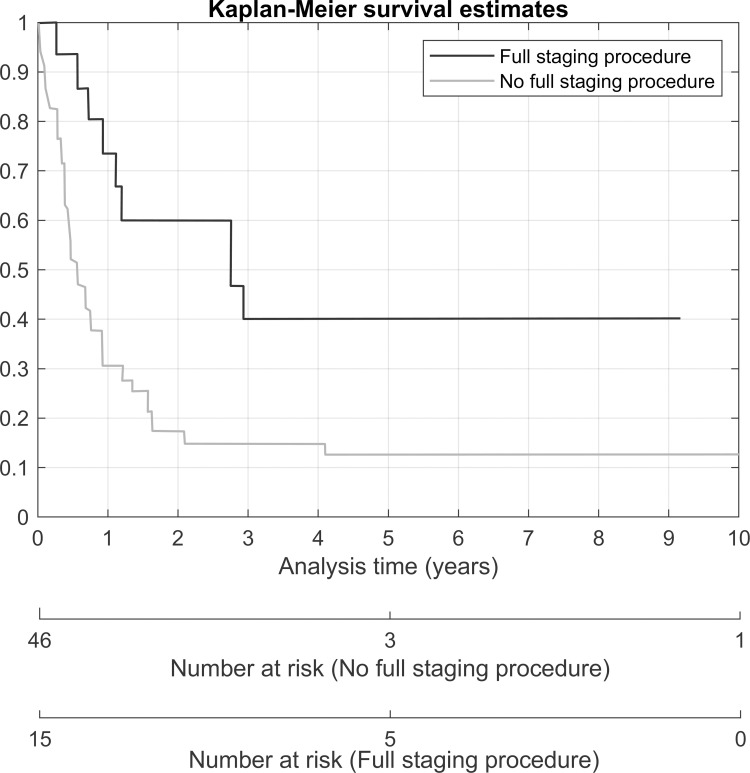
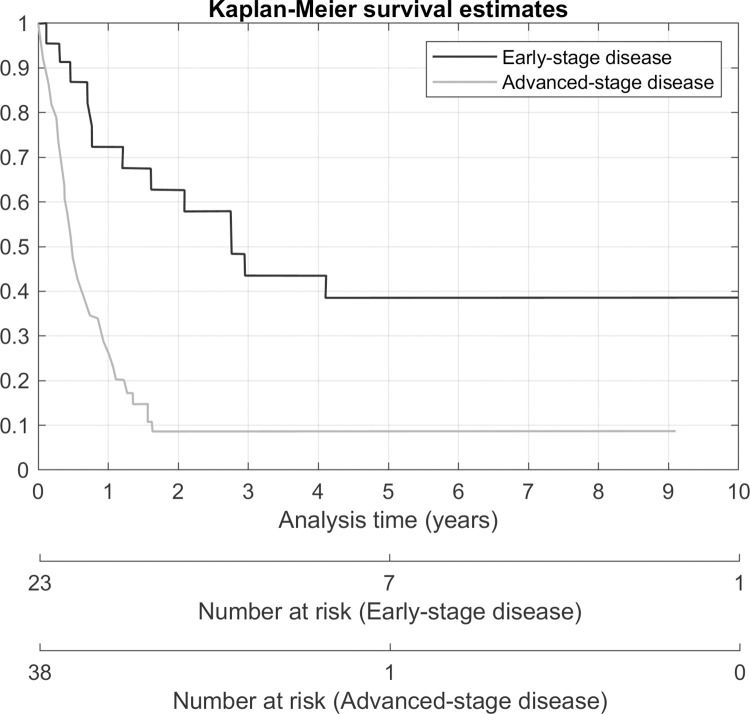
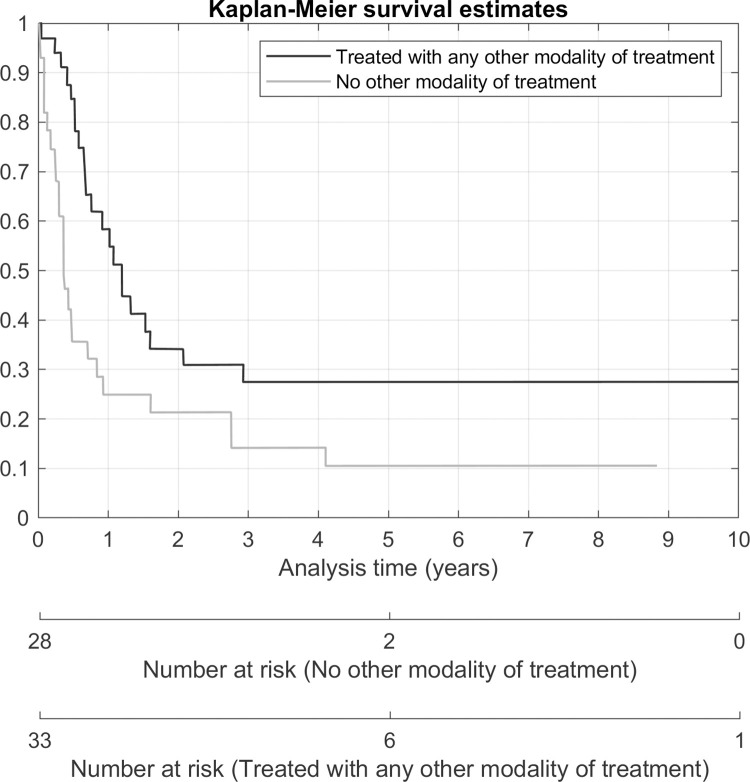
Eighteen patients (29%) presented as FIGO stage I disease, 5 patients (8%) as stage II, 16 patients (26%) as stage III and 22 patients (36%) as stage IV disease. Fifty of the 61 patients (82%) had surgery. Five-year PFS and 5-year OS were 17.3% (CI 8.9%-27.9%) and 19.7% (CI 10.6%-30.8%), respectively. Seventeen patients presented with recurrence of which 5 (29.4%) were local and 12 (70.6%) were outside the pelvis. In the univariate analysis, tumour diameter ≥ 100mm (HR 4.57; 95% CI 1.59-13.19; p-value 0.005) was associated with 5-year PFS and in univariate analysis of OS, a positive family history (HR 0.42; 95% CI 0.18-0.99; p-value 0.047), receiving a full staging operation (HR 0.37; 95% CI 0.18-0.78; p-value 0.008) and receiving any other modality of treatment, with or without surgery, (HR 0.48; 95% CI 0.27-0.85; p-value 0.012) were associated with better survival. An abnormal cervical smear (HR 2.4; 95% CI 1.03-5.6; p-value 0.041), late-stage disease (HR 3.48; 95% CI 1.79-6.77; p-value < 0.001), presence of residual tumour (HR 3.66; 95% CI 1.90-7.02; p-value < 0.001), myometrial invasion more than 50% (HR 2.29; 95% CI 1.15-4.57; p-value 0.019), cervical involvement (HR 3.38; 95% CI 1.64-6.97; p-value 0.001) and adnexal involvement (HR 3.21; 95% CI 1.56-6.63; p-value 0.002) were associated with a higher risk of death. In the multivariate analysis, full staging operation was associated with a risk of progression of disease (HR 3.49; 95% CI 1.17-10.41; p-value 0.025). Advanced stage (HR 4.2; 95% CI 2.09-8.44; p-value < 0.001) was associated with a higher risk of death. Any other modality of treatment (HR 0.28; 95% CI 0.15-0.53; p-value < 0.001) and full staging laparotomy (HR 0.27; 95% CI 0.12-0.59; p-value 0.001) was a protective factor for death.
Carcinosarcoma is an aggressive cancer with poorer survival in this specific cohort than has been described in other contemporary cohorts. Biological or genetic factors are a possible explanation for lower overall survival in this population. Although it is also possible that later diagnosis and poor access to health care contribute to poorer survival. Most recurrences occur outside of the pelvis. Full staging surgery (including pelvic lymphadenectomy) and additional use of other modalities (either for radical or palliative intent) improve survival.
本研究旨在确定患有子宫癌肉瘤患者的 5 年无进展生存期和总生存期,确定临床和手术病理特征,识别复发模式,并确定影响无进展生存期(PFS)和总生存期(OS)的预后因素。
这是一项回顾性的 10 年研究,对南非泰格伯格医院经病理证实为子宫癌肉瘤的患者进行了研究。
共研究了 61 例患者。获得了人口统计学、临床病理、治疗和结局信息。采用 Kaplan-Meier 生存分析和 Cox 比例风险模型来确定变量对 PFS 和 OS 的影响。
18 例(29%)患者为FIGO Ⅰ期疾病,5 例(8%)为Ⅱ期,16 例(26%)为Ⅲ期,22 例(36%)为Ⅳ期疾病。61 例患者中有 50 例(82%)接受了手术。5 年 PFS 和 5 年 OS 分别为 17.3%(95%CI 8.9%-27.9%)和 19.7%(95%CI 10.6%-30.8%)。17 例患者出现复发,其中 5 例(29.4%)为局部复发,12 例(70.6%)为盆外复发。在单因素分析中,肿瘤直径≥100mm(HR 4.57;95%CI 1.59-13.19;p 值 0.005)与 5 年 PFS 相关,在 OS 的单因素分析中,阳性家族史(HR 0.42;95%CI 0.18-0.99;p 值 0.047)、接受完整分期手术(HR 0.37;95%CI 0.18-0.78;p 值 0.008)和接受任何其他治疗方式,无论是否手术(HR 0.48;95%CI 0.27-0.85;p 值 0.012)与更好的生存相关。异常宫颈涂片(HR 2.4;95%CI 1.03-5.6;p 值 0.041)、晚期疾病(HR 3.48;95%CI 1.79-6.77;p 值 < 0.001)、肿瘤残留(HR 3.66;95%CI 1.90-7.02;p 值 < 0.001)、肌层浸润>50%(HR 2.29;95%CI 1.15-4.57;p 值 0.019)、宫颈受累(HR 3.38;95%CI 1.64-6.97;p 值 0.001)和附件受累(HR 3.21;95%CI 1.56-6.63;p 值 0.002)与死亡风险增加相关。在多因素分析中,完整分期手术与疾病进展的风险相关(HR 3.49;95%CI 1.17-10.41;p 值 0.025)。晚期疾病(HR 4.2;95%CI 2.09-8.44;p 值 < 0.001)与死亡风险增加相关。任何其他治疗方式(HR 0.28;95%CI 0.15-0.53;p 值 < 0.001)和完整分期剖腹手术(HR 0.27;95%CI 0.12-0.59;p 值 0.001)是死亡的保护因素。
癌肉瘤是一种侵袭性癌症,本研究特定队列的总生存期比其他当代队列描述的更差。生物学或遗传因素可能是导致该人群总体生存率较低的原因。尽管也有可能是由于晚期诊断和医疗保健获取不足导致生存率较差。大多数复发发生在盆外。完整的分期手术(包括盆腔淋巴结清扫术)和其他治疗方式的额外使用(无论是根治性还是姑息性)都可以提高生存率。