Department of Endoscopic Surgery, Sun Yat-sen University Sixth Affiliated Hospital, No. 26 Yuancun Erheng Road, Guangzhou, 510655, China.
Guangdong Provincial Key Laboratory of Colorectal and Pelvic Floor Diseases, The Sixth Affiliated Hospital, Sun Yat-sen University, Guangzhou, China.
BMC Cancer. 2022 Jul 21;22(1):806. doi: 10.1186/s12885-022-09906-5.
For colorectal cancer, preoperative (neoadjuvant) chemotherapy is more effective than postoperative chemotherapy because it not only eradicates micrometastases more effectively but also reduces the risk of incomplete intraoperative resection and tumor cell shedding. For the treatment of acute left-sided malignant colorectal obstruction, colorectal stents as well as stoma are being used to relieve the obstructive colorectal cancer, and as a bridge to surgery, allowing easy mobilization and resection of the colon. Neoadjuvant chemotherapy combined with self-expandable metal stents (SEMS) or neoadjuvant chemotherapy combined with decompressing stoma (DS) can be used as a bridge to elective surgery (BTS) as an alternative to emergency surgery in patients with acute left-sided malignant colorectal obstruction, but its benefit is uncertain. The purpose of this study was to evaluate the safety and feasibility of neoadjuvant chemotherapy as a bridge to surgery in the treatment of acute left-sided malignant colorectal obstruction.
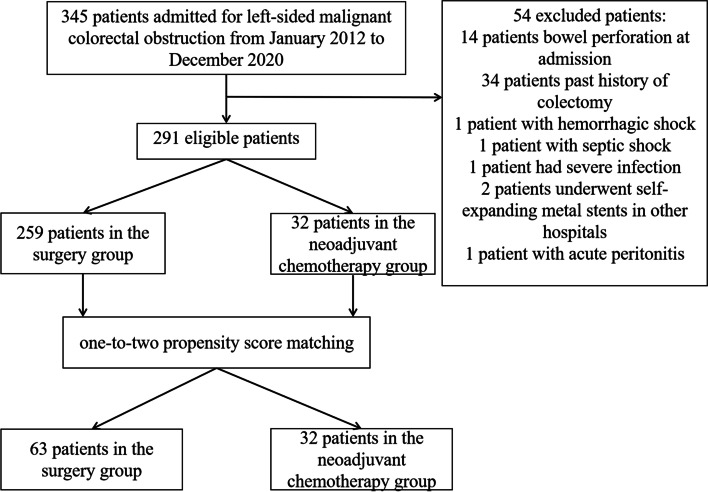
Data from patients who were admitted with acute left-sided malignant colorectal obstruction between January 2012 and December 2020 were retrospectively reviewed, and patients with gastrointestinal perforation or peritonitis were excluded. We performed one-to-two propensity score matching to compare the stoma requirement, postoperative complications, and other short-term oncological outcomes between the neoadjuvant chemotherapy group and surgery group.
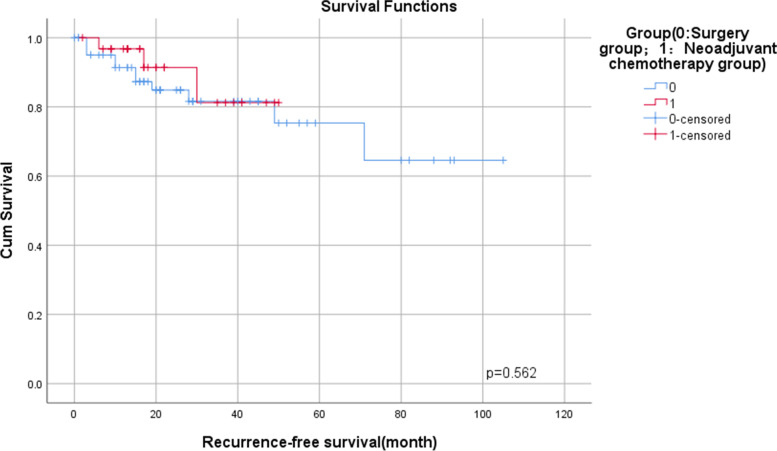
There were no differences in intraoperative blood loss, operative time, one-year postoperative mortality, and postoperative tumor markers between the two groups. The 1-year recurrence-free survival (RFS) rates of neoadjuvant chemotherapy group and surgery group were 96.8 and 91.3% (p = 0.562). The neoadjuvant chemotherapy group was able to reduce stoma rate 1 year after surgery (p = 0.047). Besides, the neoadjuvant group significantly reduced postoperative bowel function time (p < 0.001), postoperative hospital stay (p < 0.001), total hospital stay (p = 0.002), postoperative complications (p = 0.017), reduction in need to stay in the intensive care unit (ICU) (p = 0.042).
Neoadjuvant chemotherapy as a bridge to elective surgery in patients with acute left-sided malignant colorectal obstruction is safe and has many advantages. Prospective multicenter studies with large samples are needed to further evaluate the feasibility of neoadjuvant chemotherapy.
对于结直肠癌,术前(新辅助)化疗比术后化疗更有效,因为它不仅能更有效地消灭微转移灶,还能降低术中不完全切除和肿瘤细胞脱落的风险。对于急性左侧恶性结直肠梗阻的治疗,结直肠支架和造口术用于缓解梗阻性结直肠癌,并作为手术的桥梁,便于结肠的移动和切除。新辅助化疗联合自膨式金属支架(SEMS)或新辅助化疗联合减压造口术(DS)可作为急性左侧恶性结直肠梗阻患者择期手术(BTS)的桥梁,替代紧急手术,但疗效尚不确定。本研究旨在评估新辅助化疗作为急性左侧恶性结直肠梗阻手术桥梁的安全性和可行性。
回顾性分析 2012 年 1 月至 2020 年 12 月期间因急性左侧恶性结直肠梗阻入院的患者数据,排除胃肠道穿孔或腹膜炎患者。我们进行了一对一倾向评分匹配,以比较新辅助化疗组和手术组之间造口需求、术后并发症和其他短期肿瘤学结果。
两组患者术中出血量、手术时间、1 年后术后死亡率和术后肿瘤标志物无差异。新辅助化疗组和手术组的 1 年无复发生存率(RFS)分别为 96.8%和 91.3%(p=0.562)。新辅助化疗组在术后 1 年内降低了造口率(p=0.047)。此外,新辅助组明显缩短了术后肠道功能恢复时间(p<0.001)、术后住院时间(p<0.001)、总住院时间(p=0.002)、术后并发症(p=0.017)、减少入住重症监护病房(ICU)的需求(p=0.042)。
新辅助化疗作为急性左侧恶性结直肠梗阻择期手术的桥梁是安全的,具有许多优势。需要进行前瞻性多中心大样本研究进一步评估新辅助化疗的可行性。