Population, Policy and Practice Research & Teaching Department, UCL Great Ormond Street Institute of Child Health, 30 Guilford Street, London, WC1N 1EH, UK.
BMC Health Serv Res. 2022 Jul 21;22(1):936. doi: 10.1186/s12913-022-08319-1.
There is limited understanding of the drivers of increasing infant accident and emergency (A&E) attendances and emergency hospital admissions across England. We examine variations in use of emergency hospital services among infants by local areas in England and investigate the extent to which infant and socio-economic factors explain these variations.
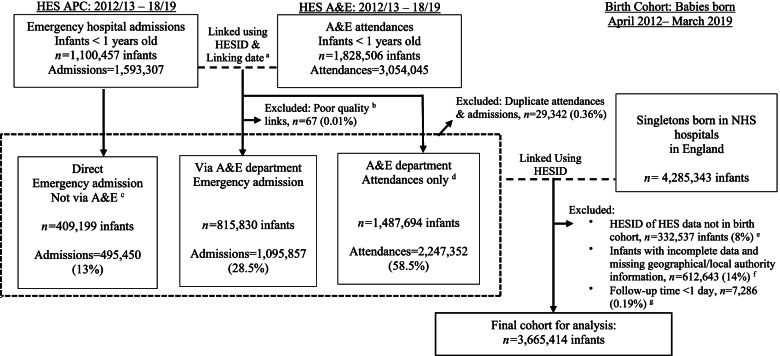
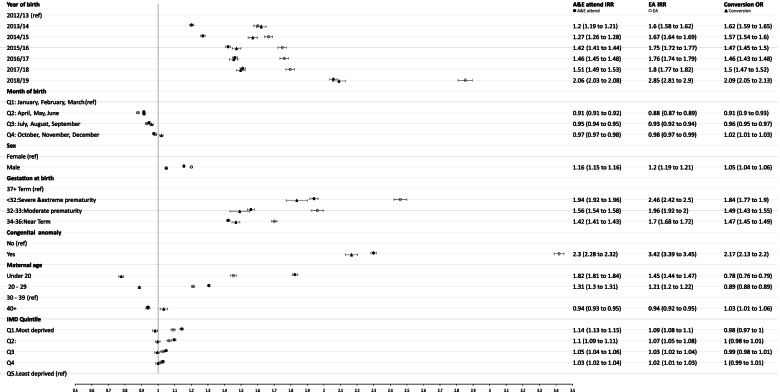
Birth cohort study using linked administrative Hospital Episode Statistics data in England. Singleton live births between 1-April-2012 and 31-March-2019 were followed up for 1 year; from 1-April-2013 (from the discharge date of their birth admission) until their first birthday, death or 31-March-2019. Mixed effects negative binomial models were used to calculate incidence rate ratios for A&E attendances and emergency admissions and mixed effects logistic regression models estimated odds ratio of conversion (the proportion of infants subsequently admitted after attending A&E). Models were adjusted for individual-level factors and included a random effect for local authority (LA).
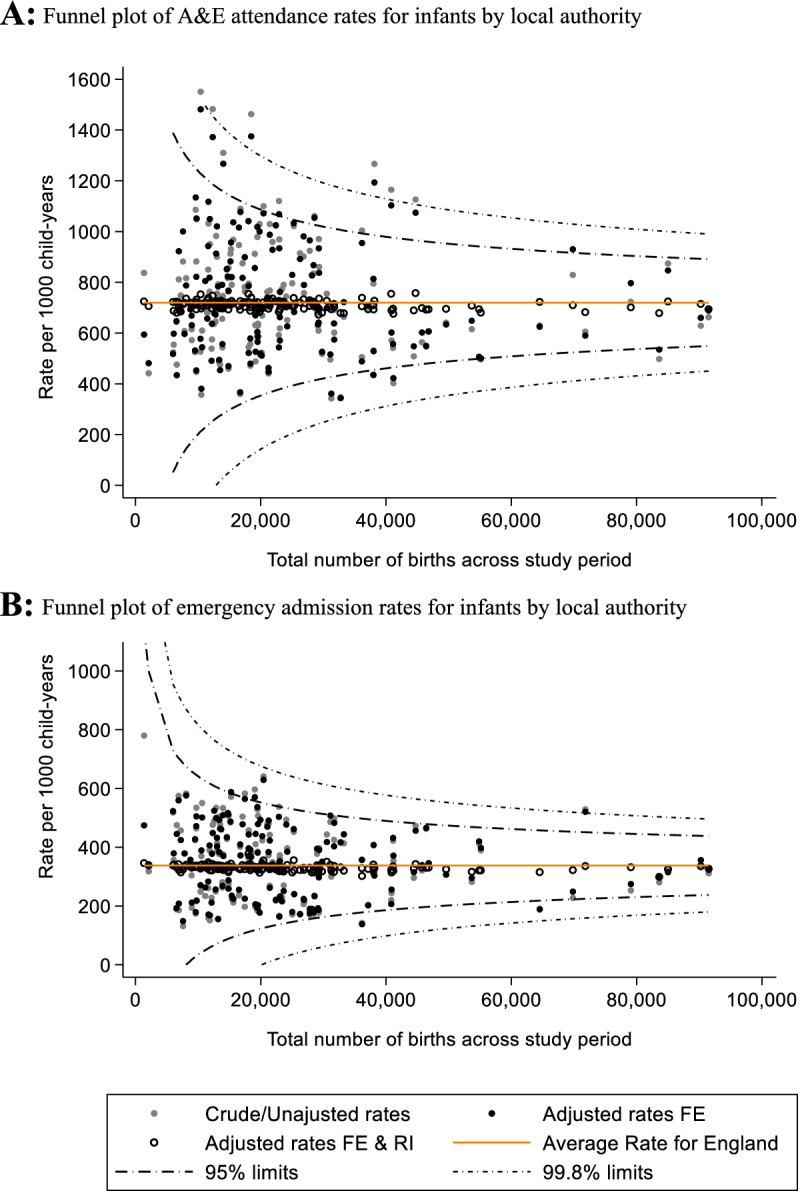
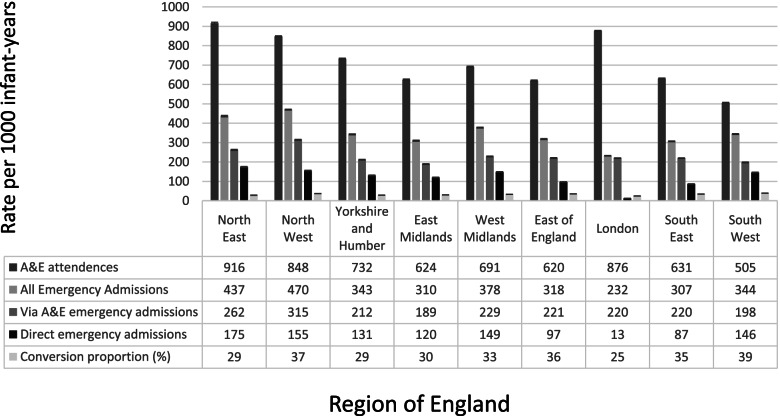
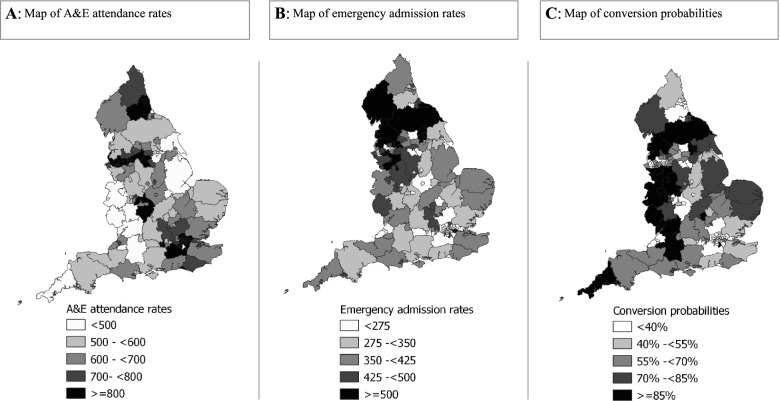
The cohort comprised 3,665,414 births in 150 English LAs. Rates of A&E attendances and emergency admissions were highest amongst: infants born < 32 weeks gestation; with presence of congenital anomaly; and to mothers < 20-years-old. Area-level deprivation was positively associated with A&E attendance rates, but not associated with conversion probability. A&E attendance rates were highest in the North East (916 per 1000 child-years, 95%CI: 911 to 921) and London (876 per 1000, 95%CI: 874 to 879), yet London had the lowest emergency admission rates (232 per 1000, 95%CI: 231 to 234) and conversion probability (25% vs 39% in South West). Adjusting for individual-level factors did not significantly affect variability in A&E attendance and emergency admission rates by local authority.
Drivers of A&E attendances and emergency admissions include individual-level factors such being born premature, with congenital anomaly and from socio-economically disadvantaged young parent families. Support for such vulnerable infants and families should be provided alongside preventative health care in primary and community care settings. The impact of these services requires further investigation. Substantial geographical variations in rates were not explained by individual-level factors. This suggests more detailed understanding of local and underlying service-level factors would provide targets for further research on mechanisms and policy priority.
目前对于英格兰不断增加的婴儿急诊就诊和急诊入院的原因还知之甚少。我们通过英格兰各地区来研究婴儿急诊服务利用的差异,并调查婴儿和社会经济因素在多大程度上解释了这些差异。
这是一项使用英格兰行政医院入院统计数据的出生队列研究。2012 年 4 月 1 日至 2019 年 3 月 31 日之间出生的单胎活产儿进行了为期 1 年的随访;从 2013 年 4 月 1 日(从出生入院的出院日期开始)到他们 1 岁生日、死亡或 2019 年 3 月 31 日。使用混合效应负二项式模型计算急诊就诊和急诊入院的发病率比值,使用混合效应逻辑回归模型估计随后转至急诊入院的转化率(即随后急诊入院的婴儿比例)。模型调整了个体水平因素,并包括地方当局(LA)的随机效应。
该队列包括 150 个英格兰地方当局的 3665414 例分娩。急诊就诊和急诊入院率最高的是:妊娠<32 周的婴儿;存在先天性异常的婴儿;母亲<20 岁的婴儿。区域贫困程度与急诊就诊率呈正相关,但与转化率无关。东北地区(916/1000 儿童年,95%CI:911 至 921)和伦敦(876/1000,95%CI:874 至 879)的急诊就诊率最高,但伦敦的急诊入院率最低(232/1000,95%CI:231 至 234),转化率最低(25%比西南部的 39%)。调整个体水平因素后,地方当局之间的急诊就诊和急诊入院率的变异性没有显著影响。
急诊就诊和急诊入院的原因包括个体水平因素,如早产、先天性异常和来自社会经济弱势的年轻父母家庭。应在初级和社区保健机构提供此类弱势婴儿和家庭的支持,并同时进行预防性保健。这些服务的影响需要进一步调查。急诊就诊率和急诊入院率的巨大地域差异不能用个体水平因素来解释。这表明,更详细地了解当地和潜在的服务水平因素将为进一步研究机制和政策重点提供目标。