Samal Lipika, D'Amore John D, Gannon Michael P, Kilgallon John L, Charles Jean-Pierre, Mann Devin M, Siegel Lydia C, Burdge Kelly, Shaykevich Shimon, Lipsitz Stuart, Waikar Sushrut S, Bates David W, Wright Adam
Division of General Internal Medicine and Primary Care, Brigham and Women's Hospital, Boston, MA.
Harvard Medical School, Boston, MA.
Kidney Med. 2022 May 28;4(7):100493. doi: 10.1016/j.xkme.2022.100493. eCollection 2022 Jul.
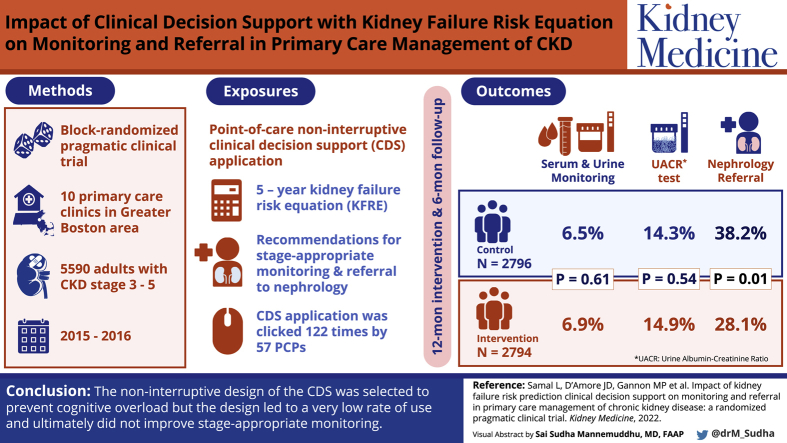
RATIONALE & OBJECTIVE: To design and implement clinical decision support incorporating a validated risk prediction estimate of kidney failure in primary care clinics and to evaluate the impact on stage-appropriate monitoring and referral.
Block-randomized, pragmatic clinical trial.
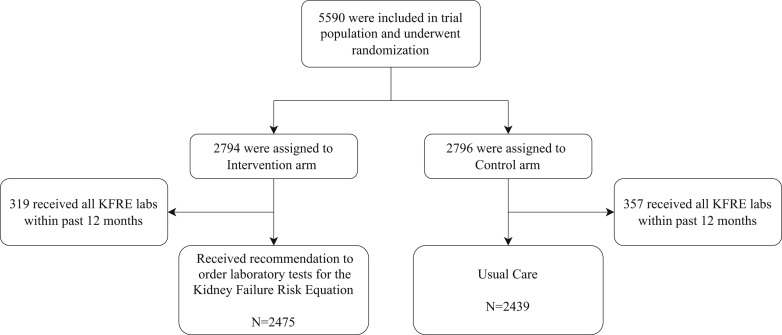
SETTING & PARTICIPANTS: Ten primary care clinics in the greater Boston area. Patients with stage 3-5 chronic kidney disease (CKD) were included. Patients were randomized within each primary care physician panel through a block randomization approach. The trial occurred between December 4, 2015, and December 3, 2016.
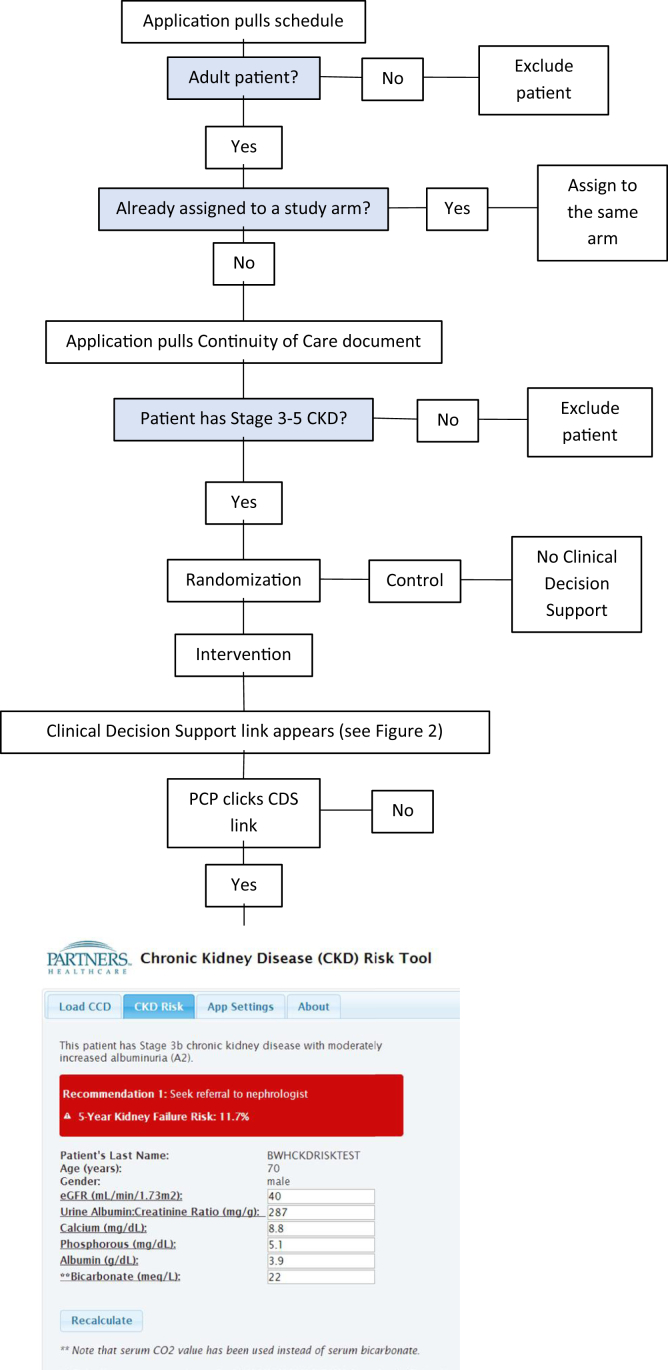
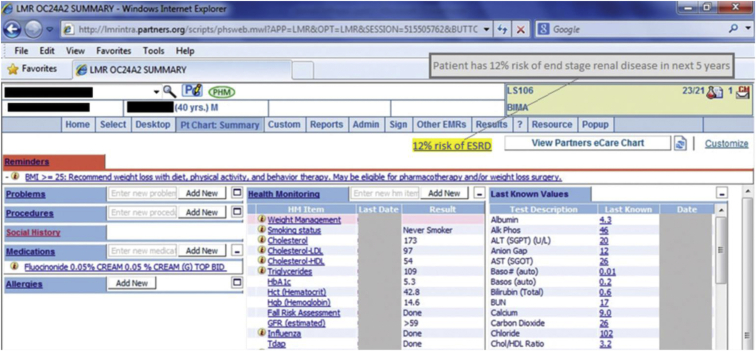
Point-of-care noninterruptive clinical decision support that delivered the 5-year kidney failure risk equation as well as recommendations for stage-appropriate monitoring and referral to nephrology.
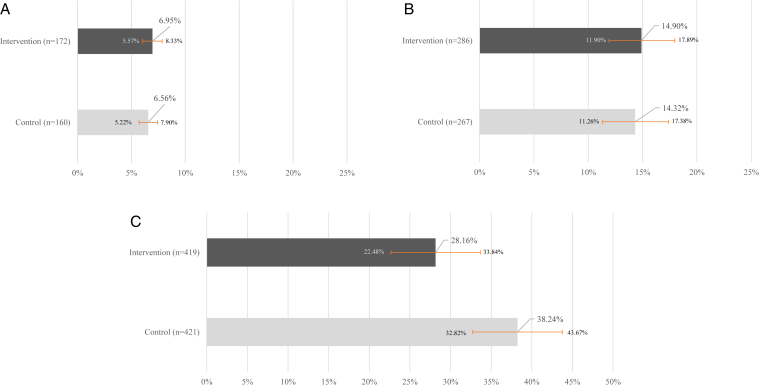
The primary outcome was as follows: Urine and serum laboratory monitoring test findings measured at one timepoint 6 months after the initial primary care visit and analyzed only in patients who had not undergone the recommended monitoring test in the preceding 12 months. The secondary outcome was nephrology referral in patients with a calculated kidney failure risk equation value of >10% measured at one timepoint 6 months after the initial primary care visit.
The clinical decision support application requested and processed 569,533 Continuity of Care Documents during the study period. Of these, 41,842 (7.3%) documents led to a diagnosis of stage 3, 4, or 5 CKD by the clinical decision support application. A total of 5,590 patients with stage 3, 4, or 5 CKD were randomized and included in the study. The link to the clinical decision support application was clicked 122 times by 57 primary care physicians. There was no association between the clinical decision support intervention and the primary outcome. There was a small but statistically significant difference in nephrology referral, with a higher rate of referral in the control arm.
Contamination within provider and clinic may have attenuated the impact of the intervention and may have biased the result toward null.
The noninterruptive design of the clinical decision support was selected to prevent cognitive overload; however, the design led to a very low rate of use and ultimately did not improve stage-appropriate monitoring.
Research reported in this publication was supported by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health under award K23DK097187.
ClinicalTrials.gov Identifier: NCT02990897.
设计并实施临床决策支持系统,纳入经验证的基层医疗诊所肾衰竭风险预测评估,并评估其对适当阶段监测和转诊的影响。
整群随机实用临床试验。
大波士顿地区的十家基层医疗诊所。纳入3 - 5期慢性肾脏病(CKD)患者。通过整群随机方法在每个基层医疗医生小组内对患者进行随机分组。试验于2015年12月4日至2016年12月3日进行。
即时护理非干扰性临床决策支持,提供5年肾衰竭风险方程以及针对适当阶段监测和转诊至肾病科的建议。
主要结果如下:在初次基层医疗就诊6个月后的一个时间点测量尿液和血清实验室监测测试结果,仅对在过去12个月内未进行推荐监测测试的患者进行分析。次要结果是在初次基层医疗就诊6个月后的一个时间点,计算得出的肾衰竭风险方程值>10%的患者转诊至肾病科。
在研究期间,临床决策支持应用程序请求并处理了569,533份连续护理文件。其中,41,842份(7.3%)文件经临床决策支持应用程序诊断为3、4或5期CKD。共有5,590例3、4或5期CKD患者被随机分组并纳入研究。57名基层医疗医生点击临床决策支持应用程序链接122次。临床决策支持干预与主要结果之间无关联。肾病科转诊存在小但具有统计学意义的差异,对照组转诊率更高。
医疗服务提供者和诊所内部的污染可能削弱了干预的影响,并可能使结果偏向无效。
选择临床决策支持的非干扰性设计以防止认知过载;然而,该设计导致使用率极低,最终并未改善适当阶段的监测。
本出版物中报告的研究由美国国立卫生研究院国家糖尿病、消化和肾脏疾病研究所根据K23DK097187号拨款资助。
ClinicalTrials.gov标识符:NCT02990897。