Ragon Institute of MGH, MIT and Harvard, Cambridge, MA.
Department of Obstetrics and Gynecology, Massachusetts General Hospital, Harvard Medical School, Boston, MA; Vincent Center for Reproductive Biology, Massachusetts General Hospital, Boston, MA.
Am J Obstet Gynecol. 2023 Jan;228(1):68.e1-68.e12. doi: 10.1016/j.ajog.2022.07.014. Epub 2022 Jul 19.
Although emerging data during the SARS-CoV-2 pandemic have demonstrated robust messenger RNA vaccine-induced immunogenicity across populations, including pregnant and lactating individuals, the rapid waning of vaccine-induced immunity and the emergence of variants of concern motivated the use of messenger RNA vaccine booster doses. Whether all populations, including pregnant and lactating individuals, will mount a comparable response to a booster dose is not known.
This study aimed to profile the humoral immune response to a COVID-19 messenger RNA booster dose in a cohort of pregnant, lactating, and nonpregnant age-matched women.
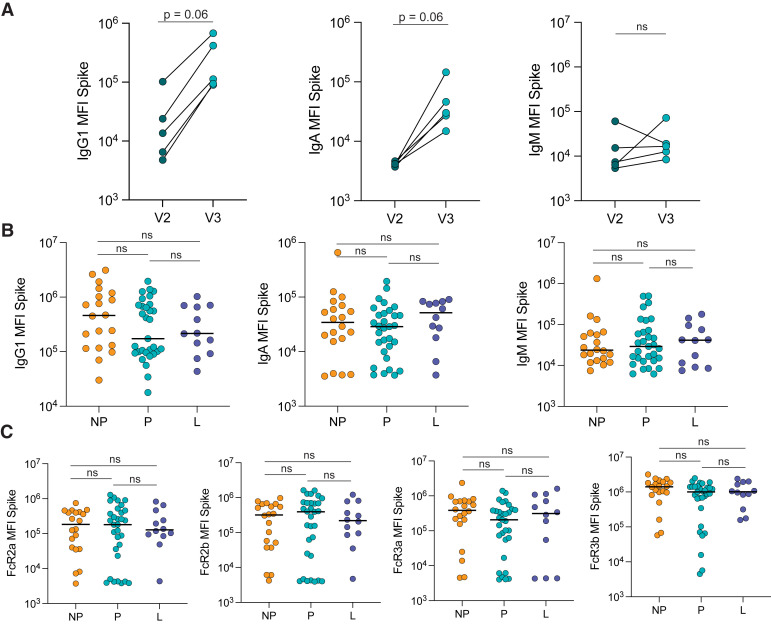
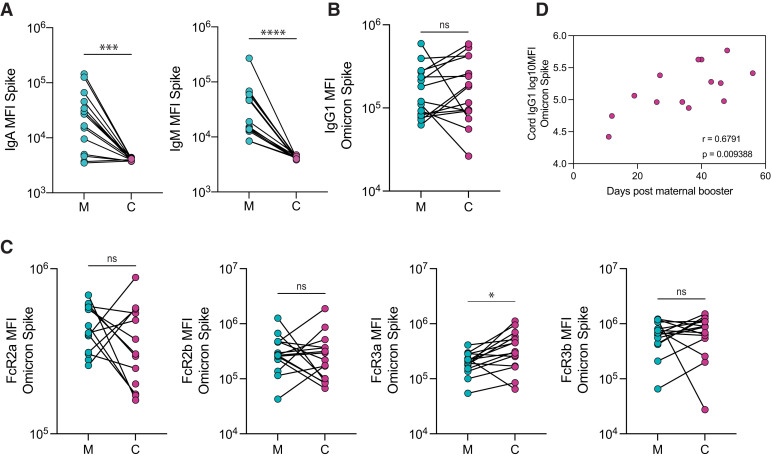
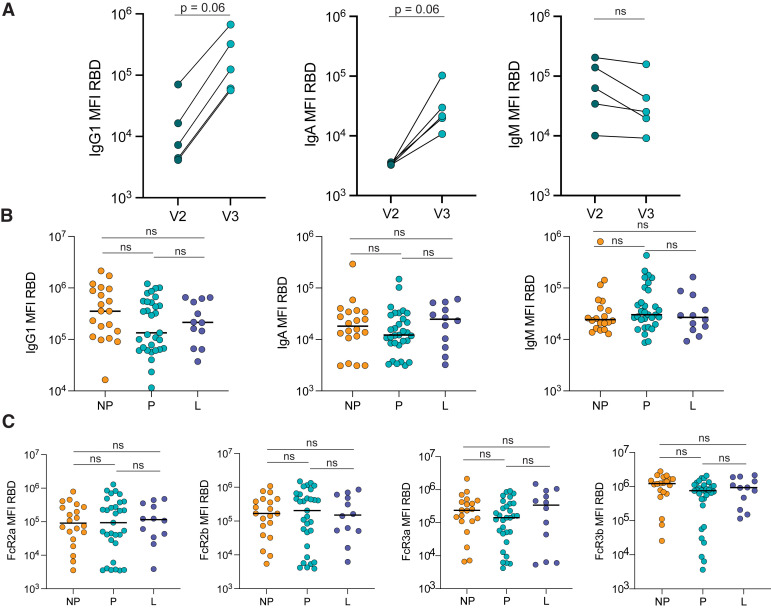
This study characterized the antibody response against ancestral Spike and Omicron in a cohort of 31 pregnant, 12 lactating, and 20 nonpregnant age-matched controls who received a BNT162b2 or messenger RNA-1273 booster dose after primary COVID-19 vaccination. In addition, this study examined the vaccine-induced antibody profiles of 15 maternal-to-cord dyads at delivery.
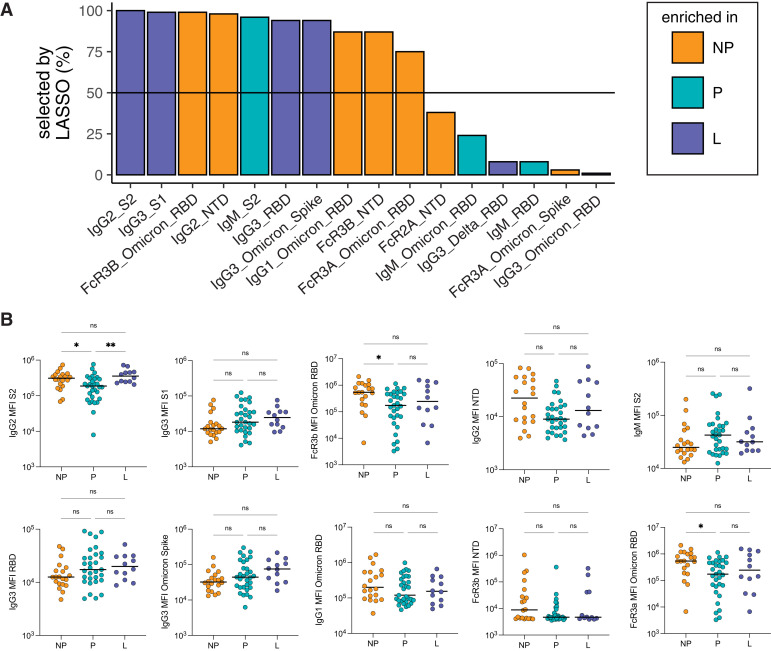
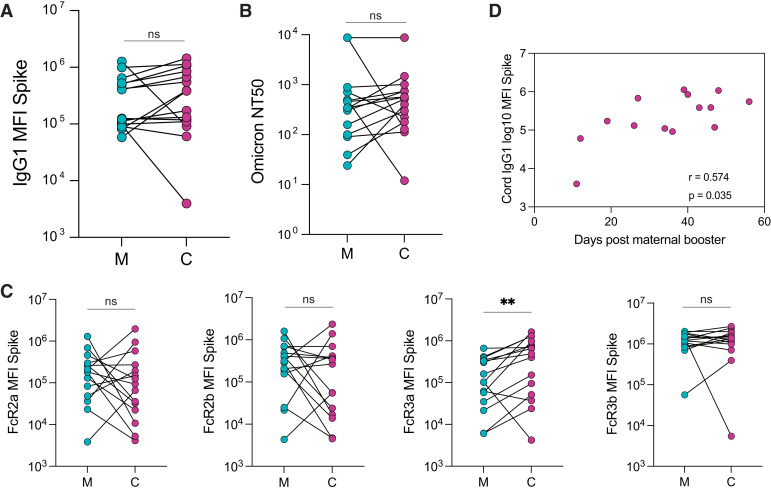
Receiving a booster dose during pregnancy resulted in increased immunoglobulin G1 levels against Omicron Spike (postprimary vaccination vs postbooster dose; P=.03). Pregnant and lactating individuals exhibited equivalent Spike-specific total immunoglobulin G1, immunoglobulin M, and immunoglobulin A levels and neutralizing titers against Omicron compared with nonpregnant women. Subtle differences in Fc receptor binding and antibody subclass profiles were observed in the immune response to a booster dose in pregnant vs nonpregnant individuals. The analysis of maternal and cord antibody profiles at delivery demonstrated equivalent total Spike-specific immunoglobulin G1 in maternal and cord blood, yet higher Spike-specific FcγR3a-binding antibodies in the cord relative to maternal blood (P=.002), consistent with the preferential transfer of highly functional immunoglobulin. Spike-specific immunoglobulin G1 levels in the cord were positively correlated with the time elapsed since receiving the booster dose (Spearman R, .574; P=.035).
Study data suggested that receiving a booster dose during pregnancy induces a robust Spike-specific humoral immune response, including against Omicron. If boosting occurs in the third trimester of pregnancy, higher Spike-specific cord immunoglobulin G1 levels are achieved with greater time elapsed between receiving the booster and delivery. Receiving a booster dose has the potential to augment maternal and neonatal immunity.
尽管在 SARS-CoV-2 大流行期间的新数据表明,信使 RNA 疫苗在包括孕妇和哺乳期妇女在内的人群中可诱导出强大的免疫原性,但疫苗诱导的免疫迅速减弱,以及令人关注的变异株的出现,促使使用信使 RNA 疫苗加强针。目前尚不清楚所有人群(包括孕妇和哺乳期妇女)对加强针的反应是否相似。
本研究旨在描述一组孕妇、哺乳期和非孕妇年龄匹配的女性接种 COVID-19 信使 RNA 加强针后的体液免疫反应特征。
本研究描述了 31 名孕妇、12 名哺乳期和 20 名非孕妇年龄匹配的对照者在初次 COVID-19 疫苗接种后接受 BNT162b2 或信使 RNA-1273 加强针后的针对原始 Spike 和奥密克戎的抗体反应。此外,本研究还检测了 15 对母婴在分娩时的脐带血样本中的疫苗诱导的抗体谱。
怀孕期间接种加强针可增加针对奥密克戎 Spike 的免疫球蛋白 G1 水平(初次接种后与接种加强针后相比;P=.03)。与非孕妇相比,孕妇和哺乳期妇女针对奥密克戎的 Spike 特异性总免疫球蛋白 G1、免疫球蛋白 M 和免疫球蛋白 A 水平以及中和滴度相当。在孕妇与非孕妇对加强针的免疫反应中,观察到 Fc 受体结合和抗体亚类谱的细微差异。在分娩时对母婴的抗体谱进行分析,结果表明在母血和脐血中均存在等效的总 Spike 特异性免疫球蛋白 G1,但在脐血中,针对 Spike 的 FcγR3a 结合抗体的水平相对母血更高(P=.002),这与高度功能性免疫球蛋白的优先转移一致。脐血中 Spike 特异性免疫球蛋白 G1 水平与接种加强针后时间的长短呈正相关(Spearman R,.574;P=.035)。
研究数据表明,怀孕期间接种加强针可诱导出强大的 Spike 特异性体液免疫反应,包括针对奥密克戎的免疫反应。如果在妊娠晚期接种加强针,则在接种加强针与分娩之间间隔时间越长,可获得更高的 Spike 特异性脐血免疫球蛋白 G1 水平。接种加强针有可能增强母婴的免疫力。